・Letter to the Editor・・Current Issue・ ・Achieve・ ・Search Articles・ ・Online Submission・ ・About IJO・
Anterior
segment optical coherence tomography for identifying muscle status in
strabismus surgery
Brijesh Takkar1, Pradeep Sharma2, Ashutosh Kumar
Singh2, Pranita Sahay2
1Vitreo Retina Services, Dr R P Centre for Ophthalmic
Sciences, All India Institute of Medical Sciences, Ansari Nagar, New Delhi
110029, India
2Pediatric Ophthalmology and Strabismus Services, Dr R P Centre for Ophthalmic Sciences, All India Institute of Medical
Sciences, Ansari Nagar, New Delhi 110029, India
Correspondence to: Pradeep Sharma. Department of Ophthalmology, Pediatric Ophthalmology and Strabismus services, Dr
R P Centre for Ophthalmic Sciences, All India
Institute of Medical Sciences, New Delhi 110029, India. drpsharma57@yahoo.com
Received: 2015-03-30
Accepted: 2015-07-22
DOI:10.18240/ijo.2016.06.26
Citation: Takkar B, Sharma P, Singh AK, Sahay P. Anterior segment optical coherence
tomography for identifying muscle status in strabismus surgery. Int J
Ophthalmol
2016;9(6):933-934
Dear Sir,
Anterior segment optical coherence tomography
(AS-OCT) finds very few indications in the domain of strabismus surgery.
Current applications remain restricted to determining limbus - muscle insertion
distance and anterior segment changes after strabismus surgery. We discuss two
cases of operated strabismus surgery where AS-OCT imaging helped in identifying
the operated eye and/or extra ocular muscles (EOM) and thus proved instrumental
in planning and management.
Case 1 A 45 years old orthotropic male presented with
post traumatic left eye rhegmatogenous retinal detachment. He had history of
strabismus surgery in the left eye in childhood for exotropia. He was planned
for left eye vitreoretinal surgery with encirclage but in the absence of
previous records, planning the encirclage was difficult. AS-OCT scans (Visante
OCT, Carl Zeiss, Germany) were ordered to identify the EOMs where both
the right and left medial rectus (MR) were found to be inserted normally. The
right MR had a smooth contour (Figure 1) while left MR appeared bulky and irregular
(Figure 2). At
similar distance of 8.85 mm from the root of the iris, right MR measured 0.42
mm in thickness (Figure 1) while left MR measured 0.60 mm (Figure 2). The
right lateral rectus (LR) appeared normal (Figure 3) while the left LR could not be identified
even on maximal left adduction. Instead shallow choroidal detachment was
identified in the left eye (Figure 4). Hence previous surgery was presumed to be
resection of left MR and supramaximal recession of left LR. During the
vitreoretinal surgery, peritomy was extended temporally for placing the
encirclage and the LR was localized at 17 mm from the limbus while MR was
normal.

Figure 1 AS-OCT image of the right eye showing
normally inserted medial rectus with smooth contour The muscle measures 0.42 mm in thickness at 8.85 mm from
the root of the iris.
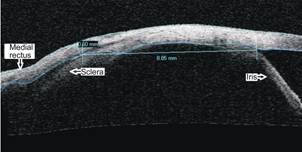
Figure 2 AS-OCT image of the left eye showing
normally inserted medial rectus The muscle is bulky with irregular contour and
measures 0.60 mm in
thickness at 8.85 mm from the root of the iris.

Figure 3 AS-OCT image of the right eye showing a
normally inserted lateral rectus with smooth contour.

Figure 4 AS-OCT image of the left eye showing
choroidal detachment Note that the lateral rectus cannot be
identified even on maximal adduction.
Case 2
A 23
years old girl presented with 30 degree exotropia in the right eye. Her father
gave history of surgery in early childhood for strabismus but could not
definitely identify the type of strabismus in childhood or the eye operated. No
records or photographs were available and bilateral bulbar conjunctiva appeared
free of scarring. With a presumptive diagnosis of consecutive right eye
exotropia, AS-OCT imaging was performed to identify EOMs. The images revealed
MR of both the eyes to be inserted normally but left MR was bulky in comparison
to right MR. The right LR was normally inserted and had a smooth contour. The
left LR however could not be identified even on maximal left adduction.
Previous strabismus surgery was again concluded as left eye LR supramaximal
recession and MR resection and the diagnoses was thus changed to residual
exotropia. She was posted for right eye surgery where intra operative findings
matched the AS-OCT findings in the right eye.
AS-OCT
imaging is non invasive, repeatable and highly reproducible for determining EOM
insertion distance from limbus[1]. We used the temporal 15 degree gaze for MR and nasal 30 degree gaze
for LR for identifying the muscles in horizontal cross sections as suggested
before[2]. Inability to localize the LR in maximal adduction was presumed to be
due to supramaximal recession in both the cases (as proven in case 1
during retinal surgery). Bulky and irregular contour of MR in both the cases
was presumed to be due to resection procedure. By identifying the operated eye
(in case 2) and the operated muscles in both the cases, AS-OCT was thus helpful
in their management and even changed our diagnoses in case 2.
AS-OCT
scanning appears consistent for the horizontal recti muscles, as in our case,
but the retro-equatorially
inserted oblique muscles are difficult to scan. Although we can quantitatively
comment on recession of the EOMs, the same cannot be done for resection
procedure and is highly subjective. For the same reason we measured thickness
of the MR in case 1 at
similar distance in both the eyes and could demonstrate higher thickness in the
operated eye (Figures 1, 2). AS-OCT has also been used to study
anterior segment changes after strabismus surgery[3-4].
To
conclude, AS-OCT is quick and effective in identifying the operated muscles in
cases of “forgotten squint surgery”. EOM recession surgeries can be objectively
identified by the same.
ACKNOWLEDGEMENTS
We thank Meena Verma, BSc (A) Optometry, for AS-OCT
imaging.
Conflicts of Interest: Takkar B, None; Sharma P, None; Singh AK, None; Sahay P, None.
REFERENCES
1 Park KA, Lee JY, Oh SY.
Reproducibility of horizontal extraocular muscle insertion distance in anterior
segment optical coherence tomography and the effect of head position. J AAPOS 2014;18(1):15-20. [CrossRef] [PubMed]
2 Liu X, Wang F, Xiao Y, Ye X, Hou
L. Measurement of the limbus-insertion distance in adult strabismus patients with
anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci 2011;52(11):8370-8373. [CrossRef] [PubMed]
3 Lüchtenberg M,
Haeussler-Sinangin Y, Kohnen T, Kuhli-Hattenbach C, Koss MJ, Schalnus R.
Changes of the anterior eye segment after eye muscle surgery-evaluation by
optical coherence tomography in adults. Klin
Monbl Augenheilkd 2010;227(10):782-785. [CrossRef] [PubMed]
4 Haeussler-Sinangin Y, Muller L, Schalnus R, Kohnen T,
Lüchtenberg M. Changes of the anterior eye segment after eye muscle
surgery-evaluation by optical coherence tomography in children. Klin Monbl Augenheilkd
2009;226(9):747-751. [CrossRef]
[PubMed]
[Top]