��Investigation����Current Issue�� ��Achieve�� ��Search Articles�� ��Online Submission�� ��About IJO�� PMC
Profitability analysis of a femtosecond laser system
for cataract surgery using a fuzzy logic approach
Jos�� AntonioTrigueros1, David P Piñero2, Mahmoud M Ismail3
1Department of
Financial Economic and Accounting, Miguel Hern��ndez
University, Elche 03202, Alicante, Spain
2Department of Optics,
Pharmacology and Anatomy, University of
Alicante, Crta San Vicente del Raspeig, Alicante 03690, Spain
3Al-Azhar University,
Cairo 11651, Egypt
Correspondence to: David P Piñero. Department of Optics, Pharmacology and Anatomy, University of Alicante, Crta San
Vicente del Raspeig s/n, San Vicente del Raspeig, Alicante 03016, Spain. david.pinyero@ua.es
Received: 2015-07-20
Accepted: 2015-10-12
Abstract
AIM: To define the financial and management conditions
required to introduce a femtosecond laser system for
cataract surgery in a clinic using a fuzzy logic approach.
METHODS: In the simulation performed in the current study, the
costs associated to the acquisition and use of a commercially available
femtosecond laser platform for cataract surgery (VICTUS, TECHNOLAS Perfect
Vision GmbH, Bausch & Lomb, Munich, Germany) during a period of 5y were
considered. A sensitivity analysis was performed considering such costs and the
countable amortization of the system during this 5y period. Furthermore, a
fuzzy logic analysis was used to obtain an estimation of the money income
associated to each femtosecond laser-assisted cataract surgery (G).
RESULTS: According to the sensitivity analysis, the femtosecond
laser system under evaluation can be profitable if 1400 cataract surgeries are
performed per year and if each surgery can be invoiced more than $500. In
contrast, the fuzzy logic analysis confirmed that the patient had to pay more per
surgery, between $661.8 and $667.4 per surgery, without
considering the cost of the intraocular lens (IOL).
CONCLUSION: A profitability of femtosecond laser systems for
cataract surgery can be obtained after a detailed financial analysis,
especially in those centers with large volumes of patients. The cost of the
surgery for patients should be adapted to the real flow of patients with the
ability of paying a reasonable range of cost.
KEYWORDS: cataract surgery;
femtosecond laser; fuzzy logic; femto-cataract; victus; profitability analysis
DOI:10.18240/ijo.2016.07.18
Citation: Trigueros JA, Piñero DP, Ismail MM. Profitability analysis of a femtosecond laser
system for cataract surgery using a fuzzy logic approach. Int J Ophthalmol 2016;9(7):1046-1050
INTRODUCTION
The introduction
of the femtosecond laser technology in cataract surgery to facilitate and
optimize the surgical procedure has supposed a great step forward[1]. Specifically, systems
based on this laser technology perform automatically some steps of the surgery,
such as the capsulorrhexis, the lens segmentation, and corneal incisions[2]. This allows a superior surgical performance compared
to conventional phacoemulsification in terms of effective phaco time[3-6] and preservation of corneal
endothelium and IOL centration[7]. This is a good addition to cataract
surgery despite it adds few remarkable advantages to experienced
phacoemulsification surgeons[8]. However, there is some controversy concerning the
cost-effectiveness of this technology and about how to make it profitable in
clinical practice[9]. The aim of this study was to define the financial and
management conditions required to introduce and make profitable a femtosecond
laser system for cataract surgery in a clinic using a fuzzy logic approach.
SUBJECTS AND METHODS
Sensitivity Analysis In the simulation performed in the current study, the
costs associated to the acquisition and use of a commercially available
femtosecond laser platform for cataract surgery during a period of 5y were
considered. Specifically, the costs corresponding to the acquisition and use of
the Victus femtosecond laser platform from Technolas Perfect Vision GmbH (Bausch & Lomb, Munich, Germany) were analyzed. Assuming a
progressive payment of this laser system in 5y, Table 1
summarizes the distribution of costs associated to the acquisition of this
laser platform.
A sensitivity
analysis was performed considering the total costs of the platform according to
Table 1. For such analysis, a 5y period was considered whether it is a
reasonable operating life for this machine. It should be remarked that this
simulation may change significantly for other different periods of evaluation. Considering this period, the countable amortization of the
femtosecond-based system was calculated which is the distribution of the costs
during the operating life of the machine.
Table 1 Summary of the
costs associated to the acquisition of the VICTUS system (Bausch & Lomb),
assuming a progressive payment in 5y
|
Payment |
Year 1 |
Year 2 |
Year 3 |
Year 4 |
Year 5 |
Total USD |
|
Down payment |
595 000 |
130 000 |
130 000 |
130 000 |
130 000 |
1 115 000 |
|
Quarterly instalments |
49 583 |
49 583 |
49 583 |
- |
- |
595 000 |
|
Monthly instalments |
17 250 |
21 563 |
25 875 |
31 238 |
37 719 |
1 603 733 |
|
Total per year |
1 000 333 |
587 083 |
638 833 |
504 850 |
582 633 |
3 313 733 |
-: No payment.
With this
sensitivity analysis, the following variables were estimated: cost per patient,
structural cost, and indirect costs associated to the activity performed with
the femtosecond machine. We considered the costs that are directly related to
the surgery and to the use of disposable materials. Finally, the total cost per
surgery was estimated.
Application of Fuzzy Logic to Estimate the Potential
Income Flow The number of patients that can attend to our clinic
requiring and/or needing for femtosecond laser-based cataract surgery is
something that cannot be known with certainty. Likewise, it is uncertain the
quantity of money that patients are ready to pay for this new modality of
cataract surgery. However, this information has a significant influence on any
type of estimation about the financial requirements for the use of femtosecond
laser-based devices. There are even intangible costs that cannot be quantified
with accuracy. Therefore, the estimation of the potential income flow due to
femtosecond laser-based cataract surgeries is uncertain and very subjective as
the evolution of the flow of patients cannot be known with certainty as well as
how technological changes will affect to the obsolescence of femtosecond
machines. For this reason, we applied the theory of fuzzy subsets to our
simulation that allow improving the quantification processes of elements that
cannot be quantified easily[10-13]. In ophthalmology, fuzzy logic has been used to
classify eye diseases[14], to analyze and classify retinal or optical coherence
tomography images[15-16], analysis of ocular movements[17], and to identify retinal exudates in diabetic
retinopathy[18]. In our study, as previous authors have done, we used
the fuzzy logic principles to define a methodology of quantification of the
intangible assets. This analysis provides more certainty to the evaluation of
the income flow due to femtosecond-based cataract surgery in an
ophthalmological clinic and allows us to define a strategy for making
profitable the use of this machine. Specifically, in
our study, we developed a sequential process subdivided in seven stages:
1) Selection of the target variable or variables. Specifically, in our
analysis the money income associated to each femtosecond laser-assisted
cataract surgery (G) was the target variable;
2) Evaluation of G by
some experts. We asked to a group of experts for an evaluation of G
considering their knowledge, experience and the information of this economic
sector. As their opinions were approximations, they were transformed into
confidence triplets;
3) First approximation of the intangible value of
G. The arithmetic mean was calculated assuming the same level of confidence for
all experts. The result was a fuzzy number informing about the approximated
achievable values for the analyzed variable;
4) Application of the expertise method. It
consists on summarizing the opinions expressed by some experts in an interval
and yielding it to a new expert evaluation. Thus, the opinions are focused
further, with a reduction of the amplitude of the interval and, therefore, of
the uncertainty and subjectivity. The results of this re-evaluation will be an
experton that will reflect the opinions of the new experts. Specifically, five
new experts performed a new evaluation using the following semantic
correspondence: 0=575.00 is correct; 0.1=practically 575.00; 0.2=almost 575.00;
0.3= close to 575.00; 0.4=closer to 575.00 rather
than to 715.00; 0.5=as close to 575.00 as to 715.00; 0.6=closer to 715.00
rather than to 575.00; 0.7=close to 715.00; 0.8=almost 715.00; 0.9=practically
715.00; and 1.0=715.00 is correct. The utilization of this methodology
facilitates to the expert the representation of the experts�� thoughts,
improving thus the sensitivity of the analysis.
Once recorded the opinions of the five experts,
the experton was built. For such purpose, the absolute frequencies, relative
frequencies and inverse accumulated frequencies were determined. As the opinions of the experts were expressed in
confidence triplets, the number of times that each value appears in the
inferior (Li) and superior (Ls) extremes of the interval, as well as in the
center of it (Vc), were determined for the estimation of absolute frequencies.
5) Calculation
of the R+-Experton. Once determined the M-Experton, the following
step was to perform its transformation into aR+-Experton, which
allowed the expression of the opinions of the experts in financial terms. 6) Calculation of the expected value of G. The mathematical expectation of the R+-Expertons were obtained and therefore an expected mean value
of the analyzed variable represented by a fuzzy number was obtained;
7) Calculation
of the final value of G.
RESULTS
Modelling and Sensitivity Analysis Table 1 summarizes the results of the sensitivity
analysis. With the data used, the mean cost per surgery was estimated to be
$524.71. Assuming that the patient paid $500, the analytical result of our
analysis was $-24.71. In other words, this equipment can be profitable if 1400
cataract surgeries are performed per year and if each surgery can be invoiced
more than $500. This analysis will allow different tests of sensitivity
considering the different situations that may happen in clinical practice.
Fuzzy Logic Analysis Six independent experts on cataract surgery (not commercially-biased)
were consulted and provided an evaluation of G, the potential money income associated to each
femtosecond laser-assisted cataract surgery in an ophthalmological clinic. Table 2 shows a summary of the results of this
consult. The expert number 1 considered that G was within the interval (600.00, 650.00), whereas the opinion of the expert number 4 was
expressed by means of a fuzzy triangular number, considering that in normal
conditions the income was $600.00 (presumption level 1), but it reached values
between (500.00, 700.00; presumption level 0) when the uncertainty
increased.
Table 2 Results of the
consultation of six independent experts on cataract surgery (not
commercially-biased) that provided an evaluation of G
|
Expert |
Evaluation of G |
Confidence triplets of G |
|
1 |
600.00, 650.00 |
[600.00, (600.00, 650.00), 650.00] |
|
2 |
550.00, 750.00 |
[550.00, (550.00, 750.00), 750.00] |
|
3 |
550.00, 700.00 |
[550.00, (550.00, 700.00), 700.00] |
|
4 |
500.00, 600.00, 700.00 |
[500.00, (600.00, 600.00), 700.00] |
|
5 |
600.00, 740.00 |
[600.00, (600.00, 740.00), 740.00] |
|
6 |
650.00, 700.00,
750.00 |
[650.00, (700.00, 700.00), 750.00] |
Assuming
the same level of confidence for all experts, the arithmetic mean of G was
calculated as follows:
M (G) =1/6��{[600.00, (600.00, 650.00), 650.00] + [550.00,
(550.00, 750.00), 750.00] + [550.00, (550.00, 700.00), 700.00] + [500.00, (600.00,
600.00), 700.00] + [600.00, (600.00, 740.00), 740.00] + [650.00, (700.00,
700.00), 750.00]} = [575.00, (600.00, 690.00), 715.00].
The result was a trapezoid fuzzy number that
estimated that the variable G will range under conditions of maximum
uncertainty in the interval (575.00, 715.00), with the maximum level of probability for the
interval (600.00, 690.00).
Table 3 summarizes the results of the re-evaluation performed by five
independent experts of the outcomes obtained in the first evaluation. The
expert number 1 considered that the intangible variable G was close to $715.00, whereas the expert number 3 estimated that G
ranged between quantities close to $715.00 and practically 715.00 (0.7= close to 715.00; 0.8= almost 715.00; 0.9= practically 715.00). Table 4 shows the experton obtained after the
analysis of the re-evaluation performed by five independent experts. As shown,
the column of absolute frequencies shows that 0.6 appeared two times as a
central value of the interval, one time as a superior extreme and another time
as an inferior extreme, whereas 0.9 appeared only one time as superior extreme
of the interval. The column of relative frequencies shows the absolute
frequencies divided by the number of experts. Finally, the column of inverse
accumulated frequencies was calculated by accumulating frequencies from the
level 1 (from bottom to top). As the opinions from experts in our study were
expressed as confidence triplets, an M-Experton was obtained, where Li is the
inferior limit, Vc is the central value and Ls is the superior limit of the
interval.
Table 3 Results of the
re-evaluation by five independent experts of the first evaluation of G
|
Expert |
Evaluation |
|
1 |
0.7 |
|
2 |
0.6 |
|
3 |
0.7, 0.8, 0.9 |
|
4 |
0.5 |
|
5 |
0.5, 0.6, 0.7 |
Table 4 Representation
of the experton n= Li/Vc/Ls
Pressumption level |
Absolute frequencies |
Relative frequencies |
Inverse accumulated frequencies |
|
0 |
0/0/0 |
0/0/0 |
1/1/1 |
|
0.1 |
0/0/0 |
0/0/0 |
1/1/1 |
|
0.2 |
0/0/0 |
0/0/0 |
1/1/1 |
|
0.3 |
0/0/0 |
0/0/0 |
1/1/1 |
|
0.4 |
0/0/0 |
0/0/0 |
1/1/1 |
|
0.5 |
2/1/1 |
0.4/0.2/0.2 |
1/1/1 |
|
0.6 |
1/2/1 |
0.2/0.4/0.2 |
0.6/0.8/0.8 |
|
0.7 |
2/1/2 |
0.4/0.2/0.4 |
0.4/0.4/0.6 |
|
0.8 |
0/1/0 |
0/0.2/0 |
0/0.2/0.2 |
|
0.9 |
0/0/1 |
0/0/0.2 |
0/0/0.2 |
|
1 |
0/0/0 |
0/0/0 |
0/0/0 |
The linear transformation of an experton, whose
data are defined in an interval (0, 1), into a R+-Experton, referenced as an
interval [A1, A2] where
A1 represents
the inferior limit of the
interval and A2 the superior limit, was performed as follows:
R+- Experton = A1 + (A2 �C A1) ��
Experton
In our study, this transformation was as follows
(Table 5):
Table 5 Representation
of the R+-M-Experton
|
Pressumptionlevel |
R+-M-Experton (Li/Vc/Ls) |
|
0 |
715.00/715.00/715.00 |
|
0.1 |
715.00/715.00/715.00 |
|
0.2 |
715.00/715.00/715.00 |
|
0.3 |
715.00/715.00/715.00 |
|
0.4 |
715.00/715.00/715.00 |
|
0.5 |
715.00/715.00/715.00 |
|
0.6 |
659.00/687.00/687.00 |
|
0.7 |
631.00/631.00/659.00 |
|
0.8 |
575.00/603.00/603.00 |
|
0.9 |
575.00/575.00/603.00 |
|
1 |
575.00/575.00/575.00 |
R+-M-Experton = 575.00 + (715.00 �C
575.00) �� M- Experton
After this, a mean value of G was obtained as follows:
E(A)= 1/10��[(715.00, 715.00, 715.00)+(715.00,
715.00, 715.00)+(715.00,
715.00, 715.00)+(715.00,
715.00, 715.00)+(715.00,
715.00, 715.00)+(659.00,
687.00, 687.00)+(631.00,
631.00, 659.00)+(575.00,
603.00, 603.00)+ (575.00,
575.00, 603.00)+(575.00,
575.00, 575.00) ]=(659.00, 664.60, 670.20).
The final result was a triangular fuzzy number that
represents the intangible income (G) that can be compared with the financial
register of a specific clinic. Figure 1 shows a graphic display of the mean
triangular fuzzy number obtained. This
number expresses that the value of G was in the interval (659.00, 670.20), with the most probable value
according to the experts of $664.60.
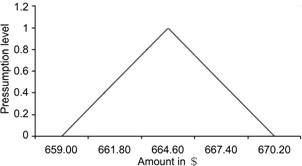
Figure 1 Fuzzy number
representing G, the potential money income associated to each
femtosecond laser-based cataract surgery in an ophthalmological clinic.
Finally, the process of fuzzy logic concluded with
the calculation of the mathematical expectation associated to the mean fuzzy
number obtained (Figure 1). Thus, the fuzzy number is transformed into a
confidence interval, eliminating the subjectivity and therefore introducing
objectivity in the estimation of the intangible evaluated.
Being A (µ) a fuzzy
number represented as a confidence interval where the level of presumption µ varies within the interval (0, 1), its
mathematical expectation
was obtained by
performing the following calculation:
As the fuzzy number was triangular in our study, its characteristic
function waslinear, and its representation by means of confidenceintervals was
as follows:
A (µ) = [(664.60
�C 659.00)�� µ + 659.00, (664.60 �C 670.20) ��µ + 670.20]
Finally, the mathematical expectation was calculated as follows:
 E[A (µ)] = [661.80, 667.40]
E[A (µ)] = [661.80, 667.40]
In summary, the fuzzy number
was transformed into a confidence interval ranging between $661.80 and $667.40.
If our sensitivity analysis revealed previously that a patient should pay $500
per femtosecond laser-assisted surgery, this fuzzy logic analysis confirms that
the patient should pay more per surgery, between $661.8 and $667.4 per surgery,
without considering the cost of the IOL.
DISCUSSION
Cataract surgery is one
of the most beneficial procedures for a patient's quality of life as it allows
a visual restoration when significant visual disturbances are present and
provides a compensation for presbyopia when multifocal IOLs are implanted.
Likewise, cataract surgery is one of the most common surgical procedures
performed and can become financially very efficient in many centers
providing cataract care[19]. However, the introduction of femtosecond laser-based systems for cataract
surgery in ophthalmological clinics and hospitals has been considered a new
challenge, as it is currently a relatively expensive technology[9]. For this reason, studies
evaluating from a management and financial perspective how to implement and
make profitable this new technology in clinical setting should be performed.
Corcoran[20] stated in a recent study that there are high
barriers to entry into the marketplace for refractive surgery and
refractive cataract surgery due to the high capital cost of excimer
and femtosecond lasers, the high skill level required to deliver
spectacular results to demanding patients who pay out of pocket, and the
necessity to perform a high volume of surgeries to satisfy both of these
requirements. In the current study, we have simulated for a specific
femtosecond laser platform for cataract surgery that is currently available in
the market which are the conditions necessary to obtain a financial benefit
with this technique after estimating the potential cash flow achievable with
this surgical procedure using fuzzy logic.
In a first sensitivity
analysis, we have obtained that the femtosecond laser system evaluated can be profitable assuming a flow of 1400 cataract
surgeries per year and a money income per surgery of more than $500, without
considering the cost of the IOL. This flow of patients may be possible in
clinics or hospitals with a great volume of patients, assuming that this
payment per surgery can be assumed by all patients. However, this cost may seem
excessive in many countries considering the conditions of the current world
economic crisis. Another question is if this cost per surgery is justified considering
the benefits of the surgery, but this was not the aim of our study. Abell and
Vote[9] performed recently a
comparative cost-effectiveness analysis
of femtosecond laser-assisted cataract surgery and
conventional phacoemulsification surgery. These authors concluded that
laser cataract surgery, irrespective of potential improvements in visual
acuity outcomes and complication rates, was not cost effective at its current
cost to patient when compared with cost-effectiveness of phacoemulsification
surgery[9]. They suggested that a significant reduction in the
cost to patient (via reduced
consumable/click cost) would increase the likelihood of femtosecond laser
cataract surgery being considered cost effective[9]. Future studies must be performed to confirm the
outcomes of this first cost-effectiveness analysis, but considering potential
future changes in the cost of these systems and considering the results of
future researches demonstrating additional advantages of femtosecond laser over
conventional phacoemulsification surgery.
The second part of our study
was the estimation by means of fuzzy logic the potential cash flow due to
patients requiring or demanding femtosecond laser cataract surgery. Considering
the opinions of different experts working in health centers with variable flow
of patients, the analysis revealed that the
patient should pay still more per surgery than in our previous estimation to
make profitable the acquisition of this technology. Specifically, the money
income per surgery should be between $661.8 and $667.4, without considering the
cost of the IOL. This suggests that the acquisition and introduction of a
femtosecond laser system for cataract surgery in any ophthalmological center
should be done on the basis of a detailed and comprehensive financial analysis
as the selection of an inappropriate cost for the surgery can lead to the
unsustainability of the equipment. It should be considered that a high price
for the surgery may ensure the profitability of the technology from a numerical
point of view, but it can suppose a significant decrease in the flow of
patients demanding the surgery and therefore can lead to a complicated
financial situation. There are many advantages of femtosecond laser cataract
surgery in terms of capsulotomy, fragmentation of the crystalline lens, corneal
wound creation, and refractive results[1-7] that have been reported in several scientific studies,
but these benefits should be also profitable in clinical practice.
In conclusion,
femtosecond laser cataract surgery can be easily profitable in clinical
practice of ophthalmological centers with large volumes of patients requiring
or demanding cataract surgery. The cost of the surgery for patients should be
adapted to the real flow of patients with the ability of paying a reasonable
range of cost. The introduction of this type of surgery in more
ophthalmological centers will depend on a potential lowering of the costs of
this technology. Finally, the correct estimation of potential cash flows is
essential for decision making in clinical practice. The use of fuzzy logic can
be very useful in these situations, allowing a more adequate estimation of
uncertain variables and allowing managers and surgeons to take more consistent
decision. The collaboration between different areas of knowledge (economy,
ophthalmology) in this type of decisions is crucial, as it cannot be only based
on technical issues.
ACKNOWLEDGEMENTS
Conflicts of Interest: Trigueros JA, None; Piñero DP, None; Ismail MM, None.
REFERENCES
1 Liu HH, Hu Y, Cui HP. Femtosecond laser in refractive
and cataract surgeries. Int J
Ophthalmol 2015;8(2):419-426. [PMC free article]
[PubMed]
2 Nagy ZZ. New technology
update: femtosecond laser in cataract surgery. Clin Ophthalmol 2014;8:1157-1167. [CrossRef] [PubMed] [PMC free article]
3 Reddy KP, Kandulla J, Auffarth GU.
Effectiveness and safety of femtosecond laser-assisted lens fragmentation and
anterior capsulotomy versus the manual technique in cataract surgery. J Cataract Refract Surg 2013;
39(9):1297-1306. [CrossRef] [PubMed]
4 Abell RG, Kerr NM, Vote BJ. Toward
zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology 2013;120(5):942-948. [CrossRef] [PubMed]
5 Abell RG, Kerr NM, Vote BJ.
Femtosecond laser-assisted cataract surgery compared with conventional cataract
surgery. Clin Experiment Ophthalmol 2013;41(5):455-462.
[CrossRef] [PubMed]
6 Conrad-Hengerer I, Hengerer FH,
Schultz T, Dick HB. Effect of femtosecond laser fragmentation on effective
phacoemulsification time in cataract surgery. J Refract Surg 2012;28(12):879-883. [CrossRef] [PubMed]
7 Conrad-Hengerer I, Al Juburi M,
Schultz T, Hengerer FH, Dick HB. Corneal endothelial cell loss and corneal
thickness in conventional compared with femtosecond laser-assisted cataract
surgery: three-month follow-up. J
Cataract Refract Surg 2013;39(9):1307-1313. [CrossRef] [PubMed]
8 Ali�� JL, Abdou AA, Puente
AA, Zato MA, Nagy Z. Femtosecond laser cataract surgery:
updates on technologies and outcomes. J
Refract Surg 2014;30(6):420-427. [CrossRef] [PubMed]
9 Abell RG, Vote BJ.
Cost-effectiveness of femtosecond laser-assisted cataract
surgery versus phacoemulsification cataract surgery. Ophthalmology 2014;121(1):10-16. [CrossRef] [PubMed]
10 Douali N, De Roo J, Sweetman P,
Papageorgiou EI, Dollon J, Jaulent MC. Personalized decision support system
based on clinical practice guidelines. Stud
Health Technol Inform 2015;211:308-310. [PubMed]
11 Alakeel AM.Using Fuzzy
Logic Techniques for Assertion-Based Software Testing Metrics. ScientificWorld Journal
2015;2015:629430. [CrossRef] [PubMed] [PMC free article]
12 Papageorgiou EI, Huszka C, De Roo J,
Douali N, Jaulent MC, Colaert D. Application of probabilistic
and fuzzy cognitive approaches in semantic web framework for medical
decision support. Comput Methods Programs
Biomed 2013;112(3):580-598. [CrossRef] [PubMed]
13 Godil SS, Shamim MS, Enam
SA, Qidwai U. Fuzzy logic: A "simple" solution for complexities
in neurosciences? Surg Neurol Int 2011;2:24.
[CrossRef] [PubMed] [PMC free article]
14 Acharya UR, Kannathal N, Ng EY, Min
LC, Suri JS. Computer-based classification of eye diseases. Conf Proc IEEE Eng Med Biol Soc
2006;1:6121-6124. [CrossRef]
15 Joshi VS, Reinhardt JM, Garvin MK,
Abramoff MD. Automated method for identification and artery-venous
classification of vessel trees in retinal vessel networks. PLoS One 2014;9(2):e88061. [CrossRef] [PubMed] [PMC free article]
16 Belghith A, Bowd
C, Weinreb RN, Zangwill LM. A joint estimation detection of Glaucoma
progression in 3D spectral domain optical coherence tomography optic nerve head
images. Proc SPIE Int Soc Opt Eng 2014;
9035:90350O.
17 Held CM, Causa J, Causa L, Est��vez
PA, Perez CA, Garrido M, Chamorro R, Algarin C, Peirano P.Automated detection
of rapid eye movements in children. Conf Proc IEEE Eng Med Biol Soc 2012;2012:2267-2270. [CrossRef]
18 Faust O, Acharya UR, Ng
EY, Ng KH, Suri JS. Algorithms for the automated detection of
diabetic retinopathy using digital fundus images: a review. J Med Syst 2012;36(1):145-157. [CrossRef] [PubMed]
19 Hansen MS, Hardten DR.
Financially efficient cataract surgery in today's healthcare
environment. Curr Opin Ophthalmol
2015; 26(1):61-65. [CrossRef] [PubMed]
20 Corcoran KJ. Macroeconomic landscape of
refractive surgery in the United States. Curr Opin Ophthalmol 2015;26(4):249-254. [CrossRef] [PubMed]
[Top]