
・Letter to the Editor・Current Issue・
・Achieve・
・Search Articles・ ・Online Submission・ ・About IJO・ PMC
Citaiton: Gatzioufas Z, Panos GD, Gkaragkani E, Georgoulas
S, Angunawela R. Recurrence of keratoconus after deep anterior lamellar
keratoplasty following pregnancy. Int
J Ophthalmol 2017;10(6):1011-1013
Recurrence of keratoconus after deep anterior
lamellar keratoplasty following pregnancy
Zisis Gatzioufas1, Georgios D. Panos2,
Evangelia Gkaragkani1, Stylianos Georgoulas1, Romesh
Angunawela1
1Moorfields Eye Hospital, London EC1V 2PD, United Kingdom
2Department of Ophthalmology, Ipswich Hospital NHS Trust, Ipswich IP4
5PD, United Kingdom
Correspondence to: Georgios D. Panos. Department of Ophthalmology, The Ipswich Hospital NHS
Trust, Heath Road, IP4 5PD, Ipswich IP4 5PD, Suffolk, United Kingdom. gdpanos@gmail.com
Received: 2016-07-02
Accepted: 2016-12-05
DOI:10.18240/ijo.2017.06.28
Citaiton: Gatzioufas Z, Panos GD, Gkaragkani E, Georgoulas
S, Angunawela R. Recurrence of keratoconus after deep anterior lamellar
keratoplasty following pregnancy. Int
J Ophthalmol 2017;10(6):1011-1013
Dear Editor,
Keratoconus is a progressive, non-inflammatory disease
of the cornea, which is characterized by marked corneal steepening and thinning[1]. It induces myopia and irregular astigmatism leading
frequently to severe visual impairment[1].
Although several aetiological factors have been implicated in its
pathophysiology, the exact mechanisms underlying keratoconus are not fully
elucidated yet. Corneal crosslinking is the treatment of choice in order to
inhibit the progression of keratoconus, whereas advanced cases require
penetrating or lamellar keratoplasty for visual restoration.
Interestingly, sporadic literature reports indicate
that keratoconus can recur in the recipient of a corneal transplant[2]. There is a number of reports on recurrence of
keratoconus following penetrating keratoplasty, including histopathological
confirmation of the disease[3-4].
Keratoconus can also recur after lamellar keratoplasty, as shown by other
groups[5-6]. However the complex
phenomenon of keratoconus recurrence remains elusive, with some authors
debating the true nature of recurrence and others suggesting potential
mechanisms that could explain the re-emergence of keratoconus[2].
Basically, it has been proposed that the re-emergence
of keratoconus after a latency period is most likely due to migration of the
disease from the host to donor cornea[7], since
keratoplasty involves only partial excision of the cornea, and recent research
evidence strongly suggests the presence of the pathology in the peripheral host
cornea[8]. Other factors such as vigorous eye
rubbing and contact lens wear have also been involved in keratoconus recurrence[2]. Nevertheless, the trigger elements that activate the
recurrence phenomenon in certain patients, have not been identified yet.
In this case report (informed consent was obtained by
the patient) we highlight a patient with keratoconus who underwent deep
anterior lamellar keratoplasty and presented recurrence of the disease after
pregnancy. Our clinical observation supports the hypothesis that hormonal
changes during pregnancy, which are involved in post-laser corneal ectasia and
may contribute to development of corneal hydrops[9-10], may also play a role in the recurrence of
keratoconus after keratoplasty.
A 23-year old female with known keratoconus attended
our clinic in December 2012. Corneal topography showed the presence of
keratoconus stage 3-4 in the right eye (OD) and keratoconus stage 3 in the left
eye (OS) (Figure 1). Her vision was 6/24 OD with rigid gas permeable contact
lenses (RGPs) and 6/12 OS with RGPs. Kmax was 61 diopters (D) OD and 58 D OS.
Corneal thinnest point was 344 microns OD and 355 microns OS. The patient had
no history of vigorous eye rubbing and was otherwise healthy. After discussion
we decided to list her for right deep anterior lamellar keratoplasty, which was
successfully performed in January 2013. Her right vision in February 2014 and
after corneal suture removal was 6/9 with RGPs. In April 2014 she underwent
penetrating keratoplasty OS (convertion to penetrating keratoplasty after
unsuccessful deep anterior lamellar keratoplasty). In January 2015 her vision
was 6/9 OD with RGPs and 6/9 OS with RGPs. During the last month of her
pregnancy the patient was experiencing gradual decrease of vision OD. She
attended our clinic in December 2015 after delivery. On slit-lamp examination
both corneal grafts were clear without any signs of rejection. However corneal
topography revealed the presence of corneal ectasia in the right corneal graft
(Figure 2), whereas the left corneal graft looked normal with mild increase of
the keratometric readings. Her vision was 6/12 OD with RGPs and 6/9 OS with
RGPs. Kmax was 54 D OD and 46 D OS. Corneal thinnest point was 422 μm OD and
508 μm OS. After discussion with the patient we decided to proceed with corneal
crosslinking OD. Her visual acuity 6mo after the treatment was 6/9 OD with RGPs
and 6/9 OS with RGPs. No signs of progression were identified until today.
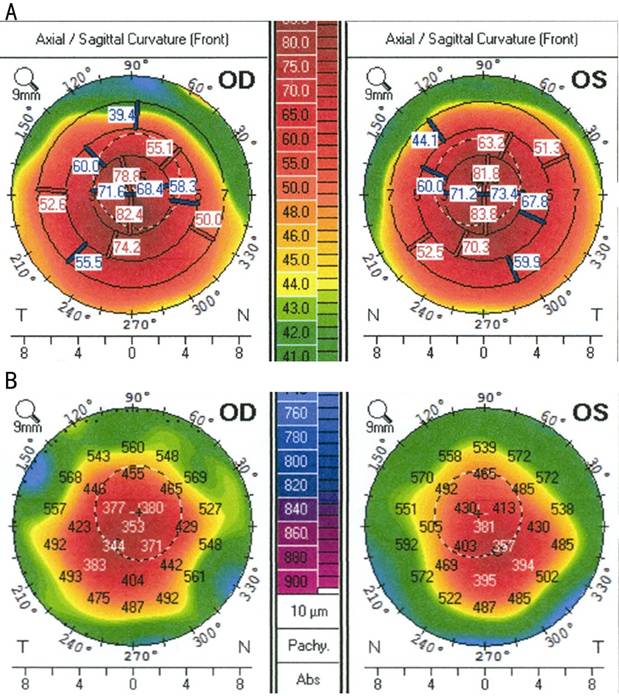
Figure 1 A: Anterior corneal curvature map derived by Pentacam, showing
keratoconus stage 3-4 in the right eye and stage 3 in the left eye; B: Corneal
thickness map showing significant corneal thinning in both eyes.
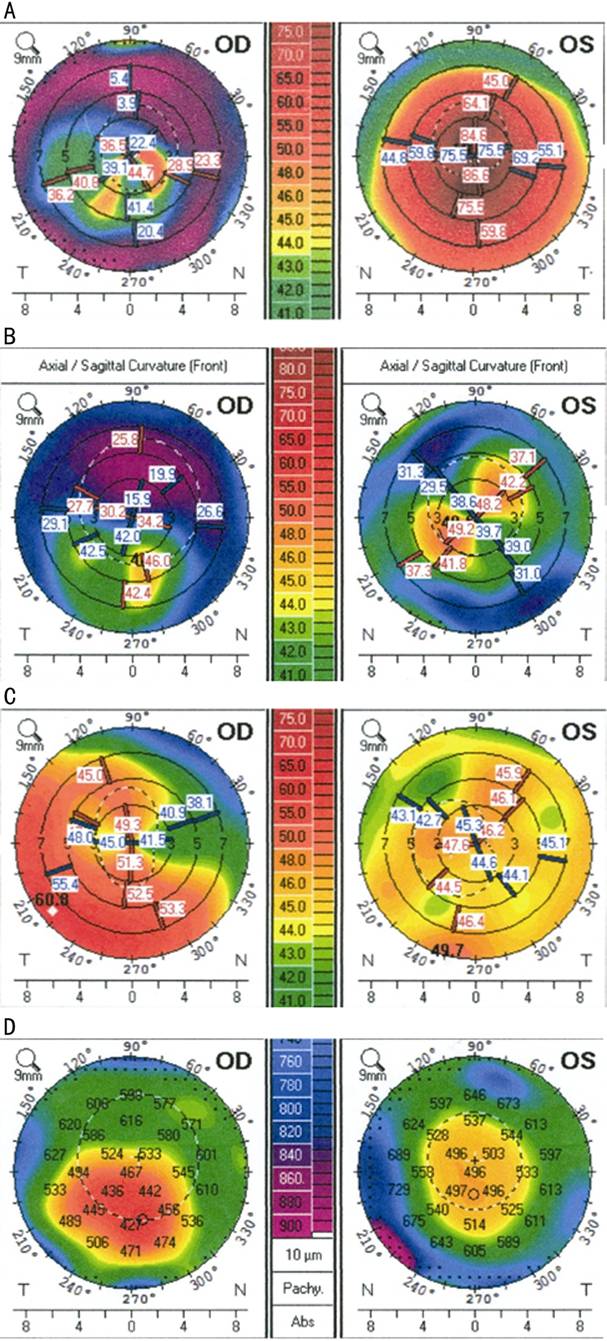
Figure 2 Corneal topography A: Anterior corneal curvature map showing irregular astigmatism after
right deep anterior lamellar keratoplasty OD in January 2013 and keratoconus
stage 3 OS; B: Corneal curvature map showing regular astigmatism after left
penetrating keratoplasty OS in April 2014 and irregular astigmatism OD; C:
Corneal curvature map showing recurrence of ectasia in the right corneal graft
OD in December 2015 and irregular astigmatism OS; D: Corneal thickness map
showing decrease of corneal thickness in the ectatic right corneal graft OD and
normal corneal thickness in the left corneal graft OS.
Recurrence of keratoconus following penetrating or lamellar keratoplasty
has been infrequently described in literature. Abelson et al[4] were first to report a histopathologically confirmed
case of keratoconus recurrence following keratoplasty. It has been hypothesized
that most recurrences of keratoconus resulted from incomplete cone excision,
but further evidence confirmed that keratoconus can re-emerge due to migration
of the pathology from host to donor cornea[2].
Interestingly the recurrence latency is considerably shorter after lamellar
keratoplasty (average 3-4y) compared to penetrating keratoplasty (average 19y)[2], supporting the clinical hypothesis that recurrences
stem from the underlying pathology in the non-excised corneal tissue. However
recurrence of keratoconus could also happen in a reverse manner, by
transplanting a donor cornea with keratoconus in a recipient requiring corneal
transplantation for reasons other than keratoconus[3].
Our patient underwent deep lamellar keratoplasty OD in
January 2013 and penetrating keratoplasty OS in April 2014. After her pregnancy
she was diagnosed with recurrence of keratoconus OD in December 2015. There is
evidence in the literature that hormonal changes occurring during pregnancy may
induce corneal ectasia after laser refractive surgery or exacerbate
pre-existing keratoconus[9-11].
Our patient was treated with corneal crosslinking OD and remained stable until
today. Her vision during her last follow-up was 6/9 OD with RGPs and 6/9 OS
with RGPs.
The early recurrence of keratoconus OD, manifesting in
the last month of pregnancy, is leading us to the conclusion that pregnancy
could have accelerated the re-emergence of keratoconus in the “vulnerable”
right cornea. The left cornea showed non-significant increase of the
keratometric readings, but no evident signs of corneal ectasia could be
detected. The latter is in agreement with the clinical observation that corneal
topographical and biomechanical variations could occur during pregnancy[12].
The exact pathophysiological mechanisms underlying the
complex interactions between hormonal influences and corneal biomechanics are
currently under investigation. However it has been suggested that high levels
of oestrogen and relaxin hormones during pregnancy, as well as the frequently
observed hypothyroxinaemia during gestation may affect corneal thickness,
corneal topography and corneal elasticity, and thereby play a role in the
development or progression of keratoconus[12-13].
This case report emphasizes on the potential risk for
re-emergence of keratoconus during or after pregnancy particularly following
lamellar keratoplasty. Physicians should be aware of this rare complication and
counsel their patients accordingly.
ACKNOWLEDGEMENTS
Conflicts of Interest: Gatzioufas Z, None; Panos GD, None; Gkaragkani E, None; Georgoulas S,
None; Angunawela R, None.
REFERENCES
1
Rabinowitz YS. Keratoconus. <ii>Surv Ophthalmol</ii>
1998;42(4):297-319. [CrossRef]
2
Bergmanson JP, Goosey JD, Patel CK, Mathew JH. Recurrence or re-emergence of
keratoconus-what is the evidence telling us? Literature review and two case
reports. <ii>Ocul Surf </ii>2014;12(4):267-272. [CrossRef]
[PubMed]
3
Unal M, Yücel I, Akar Y, Akkoyunlu G, Ustünel I, Gültekin I. Recurrence of
keratoconus in two corneal grafts after penetrating keratoplasty.
<ii>Cornea </ii>2007;26(3):362-364. [CrossRef]
[PubMed]
4
Abelson MB, Collin HB, Gillette TE, Dohlman CH. Recurrent keratoconus after
keratoplasty. <ii>Am J Ophthalmol</ii> 1980;90(5):672-676. [CrossRef]
<no>5 Feizi S,
Javadi MA, RezaeiKanavi M. Recurrent keratoconus in a corneal graft after deep
anterior lamellar keratoplasty. <ii>J Opthalmol Vis Res</ii>
2012;7(4):328-331.</no>
6
Patel N, Mearza A, Rostron CK, Chow J. Corneal ectasia following deep lamellar
keratoplasty. <ii>Br J Ophthalmol</ii> 2003;87(6):799-800. [CrossRef]
[PubMed]
7
Bourges JL, Savoldelli M, Dighiero P, Assouline M, Pouliquen Y, BenEzra D,
Renard G, Behar-Cohen F. Recurrence of keratoconus characteristics: a clinical
and histologic follow-up analysis of donor grafts. <ii>Ophthalmology
</ii>2003;110(10):1920-1925. [CrossRef]
8
Mathew JH, Goosey JD, Bergmanson JP. Quantified histopathology of the
keratoconic cornea. <ii>Optom Vis Sci</ii> 2011;88(8):988-997. [CrossRef]
[PMC free
article] [PubMed]
9
Padmanabhan P, Radhakrishnan A, Natarajan R. Pregnancy-triggered iatrogenic
(post-laser in situ keratomileusis) corneal ectasia-a case
report.<ii>Cornea</ii> 2010;29(5):569-572. [CrossRef]
[PubMed]
10
Gatzioufas Z, Thanos S. Acute keratoconus induced by hypothyroxinemia during
pregnancy. <ii>J Endocrinol Invest</ii> 2008;31(3):262-266. [CrossRef]
[PubMed]
11
Hafezi F, Iseli HP. Pregnancy-related exacerbation of iatrogenic keratectasia
despite corneal collagen crosslinking. <ii>J Cataract Refract
Surg</ii> 2008;34(7):1219-1221. [CrossRef]
[PubMed]
12
Hoogewoud F, Gatzioufas Z, Hafezi F. Transitory topographical variations in
keratoconus during pregnancy. <ii>J Refract Surg</ii> 2013;29(2):
144-146. [CrossRef]
[PubMed]
13
Spoerl E, Zubaty V, Raiskup-Wolf F, Pillunat LE. Oestrogen-induced changes in
biomechanics in the cornea as a possible reason for keratectasia. <ii>Br
J Ophthalmol</ii> 2007;91(11):1547-1550. [CrossRef]
[PMC free
article] [PubMed]