
・Letter to the Editor・Current Issue・ ・Achieve・ ・Search Articles・ ・Online Submission・ ・About IJO・ PMC
Citation: Hwang KY, Lim SA, Chung SH. A case of
hypermature cataract formation following implantation of an implantable
collamer lens with an Aquaport. Int J Ophthalmol 2017;10(6):1014-1015
A case of hypermature cataract formation following
implantation of an implantable collamer lens with an Aquaport
Kyu-Yeon Hwang1, Sung A. Lim2,
So-Hyang Chung3
1Department of Ophthalmology, Konyang University, Kim’s Eye
Hospital, Seoul 07301, Korea
2Nune Eye Hospital, Daegu 42019, Korea
3Department of Ophthalmology and visual science, Seoul St. Mary's
Hospital, College of Medicine, the Catholic University of Korea, Seoul 06591,
Korea
Correspondence
to: So-Hyang Chung. Department of Ophthalmology and visual science,
Seoul St. Mary’s Hospital, College of Medicine, the Catholic University of
Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea. chungsh@catholic.ac.kr
Received:
2016-07-04
Accepted: 2016-11-02
DOI:10.18240/ijo.2017.06.29
Citation: Hwang KY, Lim SA, Chung SH. A case of
hypermature cataract formation following implantation of an implantable
collamer lens with an Aquaport. Int J Ophthalmol 2017;10(6):1014-1015
Dear
Editor,
To
improve humor circulation the latest V4c Visian implantable collamer lens (ICL)
was designed with a 0.36-mm Aquaport[1-2]. This design also
eliminates the need to perform peripheral iridectomy before ICL implantation.
Several authors reported rates of secondary surgical intervention related to
insufficient vault in the presence or absence of cataract formation and
excessive vault in the presence or absence of elevated intraocular pressure
(IOP) after ICL insertion[1]. Here, we report a case of rapid
progression of a cataract to a hypermature state after implantation of an ICL
with an Aquaport.
A
29-year-old man, who had undergone implantation of bilateral ICLs with an
Aquaport at another eye clinic 4mo earlier, was referred to our hospital with a
complaint of progressive blurring of vision in the left eye. The white-to-white
diameter of his left eye by caliper was 12 mm and the size of implanted ICL was
12.6 mm. The ICLs had been inserted at a superior corneal incision. Uncorrected
distance visual acuity (UDVA) in both eyes was 20/20 on postoperative day 7,
and his medical records showed no intraoperative surgical complications.
On
his initial visit to our clinic, the right eye had normal vision and no
cataract formation. The best spectacle-corrected visual acuity (BCVA) in the
left eye was 20/50, and slit-lamp examination showed an anterior subcapsular
opacity and swelling of the lens. The vaulting of the ICL was three quarters of
the corneal thickness in the right eye and one quarter in the left eye. The
Aquaport was well centered in the right eye and ICL wasdecentered inferonasally
and in a vertical position in the left eye. The anterior chamber was clear in
both eyes (Figure 1). Figure 2 shows the Pentacam Scheimpflug image of left
eye. After one month, the subcapsular opacity progressed rapidly to a
hypermature cataract in the left eye and the ICL was rotated to 60 degrees from
the horizontal meridian (Figure 3). There was flare of 1+ in the anterior
chamber of the left eye. BCVA was determined by hand motion. We immediately
performed cataract surgery and removed the ICL and inserted anAcri LISA®
(Carl Zeiss Meditec., Oberkochen, Germany) intraocular lens under the
anterior capsule with staining by indocyanine green (ICG) dye in the left eye.
The lens capsule under ICG staining was intact and no perforation was observed.
On the first postoperative day, UDVA was 20/25 and uncorrected near visual
acuity (UNVA) was J2. The pro-inflammatory cytokine interleukin 6 (IL-6) in the
anterior chamber that was obtained during surgery was 69.6 pg/mL by ELISA
(normal values, 0-46 pg/mL). Slit-lamp examination demonstrated whitish
infiltrates on the ICL surface (Figure 4). At 3mo after surgery, UDVA was 20/20
and UNVA was J2. There was no inflammatory reaction in the anterior chamber.
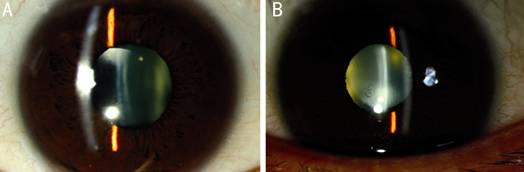
Figure
1 Slit lamp findings of right (A) and left (B) eyes at initial visit.
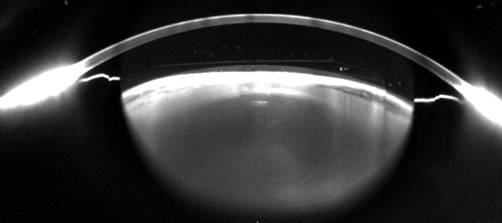
Figure
2 Pentacam Scheimpflug image of left eye.
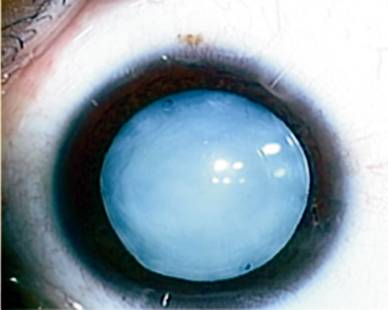
Figure
3 Hypermature cataract at surgery.
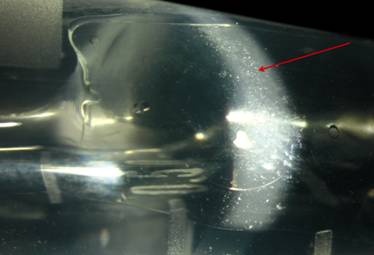
Figure
4 Whitish infiltrates on explanted ICL surface by slit lamp microscopy.
Several
studies of ICLs with Aquaport reported low postoperative complication rates
compared with conventional ICLs due to the possible flow of the aqueous humor
through the Aquaport[3-5]. In a literature review of 2592 eyes, the
occurrence of cataract formation with the latest ICL models without Aquaport
was 5.2%[6]. Most cataracts were reported as nonprogressive or
slowly progressive and asymptomatic and were placed under surveillance.
The
patient who presented at our clinic had a cataract that rapidly progressed to
the hypermature state within 1mo. Five months earlier he had ICL with Aquaport
implantation in both eyes. Rapid progression cataract within 1mo has not been
reported even in conventional ICL cases. According to the patient’s medical records, the
preoperative anterior chamber depth was 3.05 mm and there were no
intraoperative complications such as the lens touching the cornea or intraoperative
bleeding due to inadequate manipulation. Gradual subcapsular opacity and
swelling of the lens was detected at presentation. During cataract surgery, the
lens capsule was shown to be intact under ICG staining, indicating no
penetrating trauma to the lens capsule when the ICL was implanted.
The
reason for the rapid cataract progression in an eye with an ICL and Aquaport is
not clear. A low vault and decentration of an Aquaport might lead to
disturbances in the aqueous flow, interfering with lens nutrition and causing
metabolic disturbances to the crystalline lens[6-7]. Although
Aquaport improve circulation of aqueous humor to the anterior surface of the
crystalline lens, the rapid flow might lead to rapid progression of cataracts,
especially in low vaulting cases. Kawamorita et al[2] showed that
the flow velocity 0.25 mm in front of the center of the crystalline lens was
1.52×10-1 mm/s for an ICL with an Aquaport and 1.21×10-5
mm/s for a conventional ICL. Finally, a decentered Aquaport might prevent
adequate circulation of the aqueous humor and increase the pro-inflammatory
cytokine IL-6 in the anterior chamber and whitish infiltration on the ICL
surface.
This
case of rapid progression of a cataract in a patient with an ICL with an
Aquaport shows the need for close monitoring to detect rapid progression of
cataracts after ICL implantation.
ACKNOWLEDGEMENTS
Foundation: Supported
by the National Research Foundation of Korea (NRF) grant funded by the Korea
government (MSIP) (No.2017R1A2B4012327).
Conflicts
of Interest: Hwang KY, None; Lim SA, None; Chung SH,
None.
REFERENCES
1 Packer M.
Meta-analysis and review: effectiveness, safety, and central port design of the
intraocular collamer lens. <ii>Clin Ophthalmol
</ii>2016;10:1059-1077. [CrossRef] [PMC free article] [PubMed]
2 Kawamorita T,
Uozato H, Shimizu K. Fluid dynamics simulation of aqueous humour in a
posterior-chamber phakic intraocular lens with a central perforation.
<ii>Graefes Arch Clin Exp Ophthalmol </ii>2012;250(6):935-939. [CrossRef]
[PubMed]
3 Shimizu K, Kamiya
K, Igarashi A, Shiratani T. Early clinical outcomes of implantation of
posterior chamber phakic intraocular lens with a central hole (Hole ICL) for
moderate to high myopia. <ii>Br J Ophthalmol</ii>
2012;96(3):409-412. [CrossRef] [PubMed]
4 Kamiya K, Shimizu
K, Saito A, Igarashi A, Kobashi H. Comparison of optical quality and
intraocular scattering after posterior chamber phakic intraocular lens with and
without a central hole (Hole ICL and Conventional ICL) implantation using the
double-pass instrument. <ii>PLoS One</ii> 2013;8(6):e66846. [CrossRef] [PMC free article] [PubMed]
5 Shimizu K, Kamiya
K, Igarashi A, Shiratani T. Intraindividual comparison of visual performance
after posterior chamber phakic intraocular lens with and without a central hole
implantation for moderate to high myopia. <ii>Am J Ophthalmol
</ii>2012;154(3):486-494.e1. [CrossRef]
[PubMed]
6 Fernandes P,
Gonzalez-Meijome JM, Madrid-Costa D, Ferrer-Blasco T, Jorge J, Montes-Mico R.
Implantable collamer posterior chamber intraocular lenses: a review of
potential complications. <ii>J Refract Surg</ii>
2011;27(10):765-776. [CrossRef] [PubMed]
7 Shiratani T,
Shimizu K, Fujisawa K, Uga S, Nagano K, Murakami Y. Crystalline lens changes in
porcine eyes with implanted phakic IOL (ICL) with a central hole.
<ii>Graefes Arch Clin Exp Ophthalmol</ii> 2008;246(5):719-728. [CrossRef]
[PMC free article] [PubMed]