
・Letter to the Editor ・ Current
Issue IF in JCR CiteScore ・Submission・ In Press Recent Accepted PMC RSS
・・
Citation: Cennamo
G, Romano MR, Breve MA, Velotti N, de Crecchio G, Cennamo G. Optical coherence
tomography-angiography of juxtapapillary hamartoma. Int J Ophthalmol 2017;10(8):1328-1330
Optical coherence tomography-angiography of
juxtapapillary hamartoma
Gilda Cennamo, Mario R Romano, Maria Angelica
Breve, Nunzio Velotti, Giuseppe de Crecchio, Giovanni Cennamo
Department of Neurosciences, Reproductive Sciences and Dentistry, Eye
Clinic, University of Naples Federico II, Via S.
Pansini 5, Naples 80133, Italy
Correspondence to: Gilda Cennamo. Department of Neurosciences, Reproductive
Sciences and Dentistry, Eye Clinic, University of Naples Federico II, Via S. Pansini 5, Naples 80133, Italy. xgilda@hotmail.com
Received:
2016-09-16 Accepted: 2016-12-16
DOI:10.18240/ijo.2017.08.23
Citation: Cennamo
G, Romano MR, Breve MA, Velotti N, de Crecchio G, Cennamo G. Optical coherence tomography-angiography
of juxtapapillary hamartoma. Int
J Ophthalmol 2017;10(8):1328-1330
Dear
Editor,
I’m
Dr. Gilda Cennamo from the Eye Clinic of Department of Neurosciences,
Reproductive Sciences and Dentistry, University of Naples Federico II, Naples,
Italy. I write to present four cases of juxtapapillary hamartoma evaluated with
non-invasive optical coherence tomography-angiography (OCT-A).
The
term “hamartoma” was coined by Albrecht[1] in 1904
to describe a group of benign tumor-like malformations arising from deranged
mixing or deranged development of normal tissue in an organ. Hamartomas of the
retina, the retinal pigment epithelium (RPE) are characterized by a mound of
disorganized glial, vascular and melanocytic tissue; these alterations are also
found in the papilla[2].
Spectral-domain
optical coherence tomography (SD-OCT) of combined hamartoma of the retina and
RPE shows an elevated pigmented mass that is commonly connected to the
epiretinal membrane[3] but does not adequately
image the vascular compartment. In this scenario, we evaluated the vascular
features of juxtapapillary hamartomas in four patients using non-invasive
OCT-A.
In
this prospective study we evaluated four eyes of four patients affected by juxtapapillary hamartoma seen in the Eye Clinic of the University
of Naples Federico II between September 2015 and December 2015. The study protocol was approved by the Institutional Review Board of the
University of Naples Federico II, and adhered to the tenets of the Declaration
of Helsinki. No patient had coexisting systemic neurofibromatosis type 1 or 2.
Each patient underwent evaluation of best corrected
visual acuity (BCVA) according to the Early Treatment of Diabetic Retinopathy
Study (ETDRS), A-scan and B-scan bulbar echography (Quantel Medical,
Clermont-Ferrand, France), multicolor imaging,
SD-OCT
and fluorescein and indocyanine angiography (Spectralis HRA+, Heidelberg
Engineering, Heidelberg, Germany), widefield
en-face OCT and OCT-A (Optovue AngioVue System, Optovue Inc., Fremont, CA, USA).
OCT-A
has an A-scan rate of 70 000 scans
per second with a tissue axial resolution of 5 μm and a 15-μm beam width, each
B-scan contained 304 A-scans. This new technique analyzes blood flow through
the “split spectrum amplitude decorrelation” algorithm: blood flowing through
vessels changes reflectance over time and localized areas of flow decorrelation
between frames. The spectrum of the light source
was split in multiple component parts to decrease the noise of images and then
decorrelation was carried out to obtain an image of the contained blood flow[4].
The
tumor area was measured with a 3×3 scan centered on the optic
disc. We evaluated, simultaneously, the superficial vascular plexus, the deep
vascular plexus, the outer retina and the RPE area (choroidal cup)
The median age of our four patients at
diagnosis was 13.7y, and three were male. The BCVA of affected eyes was 0.1 logMAR to
counting finger secondary to severe retinal disorganization and loss of photoreceptors
in the macular region. All tumors involved the optic nerve. In three of the
four patients, the tumor was located in the left eye. Multicolor images showed
a green lesion at the level of the optic disc (Figures 1A, 2A). At standardized A-scan
echography, the mean tumor basal dimension was 2.98 mm. SD-OCT examination showed retinal fluid in three affected eyes,
retinal striae overlying the tumor in two eyes, retinal schisis in two eyes and
vitreo-retinal traction in all eyes (Figures 1E, 2H).
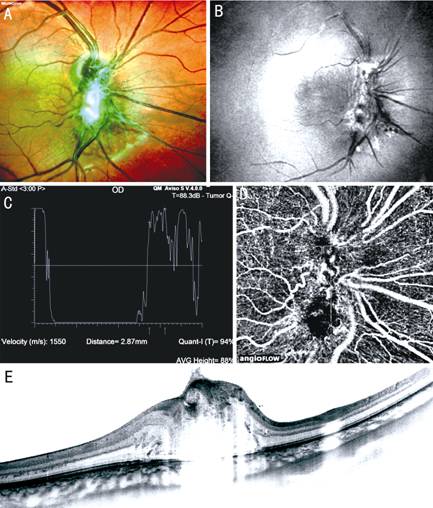
Figure 1 Juxtapapillary hamartoma in the left
eye of a 8-year-old boy A: Multicolor
image of the lesion; B: En-face
widefield OCT revealed retinal folds emanating from the tumor; C: A-scan echography showing eye reflectivity in the internal part
of the lesion; D: OCT
angiography revealed vascular tortuosity and rarefied capillaries; E: SD-OCT scans through the tumor show retinal thickness, horizontal
and vertical traction.
Widefield
en-face OCT revealed epiretinal membranes in all four patients: in two with
foveal involvement, in one with extrafoveal involvement, and in two with both
foveal and extrafoveal involvement. Vitreo-retinal traction was horizontal
(tangential) in one patient, vertical (anteroposterior) in one patient, and
both horizontal and vertical in two patients (Figure 1B). Early phase
fluorescein and indocyanine angiography images showed fine vascularization in
the center of the tumor and numerous anastomotic vessels, which were not
visible in the later phase due to die leakage (Figure 2). Moreover, fluorescein
angiography revealed ophthalmoscopic modifications of vessels and of the optic
disc, characterized by an increase of fluorescein in the centre of the lesion
due to the permeability of capillaries (Figures 2B-2E). OCT-A showed a series
of vascular irregularities, namely, dilatation and vascular tortuosity and
rarified capillaries (Figures 1D, 2F and 2G).
Clinically,
the differential diagnosis of juxtapapillary hamartoma is with choroidal
melanoma, retinoblastoma and neoplasm of the optic nerve with endobulbar
manifestation. Gass[6] reported the
histopathological features of these lesions as follows: thickening of the
retina and optic nerve due to replacement of the normal architecture of the
retina and optic nerve by dysplastic glial vascular tissue infiltrated by
cords, strands and sheets of pigment epithelial cells; a sheet of fibrous
tissue proliferation bridging the folded anterior surface of the lesion; and an
unusual pattern of dilated capillaries. Hamartomas gradually lead to visual
deficiency, but they never evolve to malignancy[7].
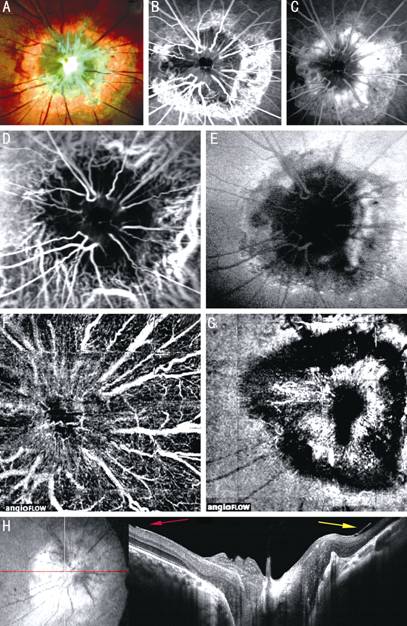
Figure
2 Juxtapapillary hamartoma in the left eye of a 22-year-old man A: Multicolor image of the tumor; B, C:
Early and late phase fluorescein angiography showing fine vascularization in
the center of the neoformation and numerous anastomotic vessels; D, E: Early
and late phase indocyanine angiography show vascular tortuosity; F, G: OCT
angiography of the superficial and deep capillary network reveals vascular
irregularities within the tumor; H: SD-OCT scans through the tumor shows
horizontal traction (red arrow) and vertical traction (yellow arrow).
In
our study, standardized A-scan echography showed a lesion with high
reflectivity (about 85%) without acoustic shadowing, thereby excluding both
malignant melanoma and retinoblastoma, and indicating an angiomatous
malformation. Fluorescein angiography images showed modifications of vessels in
the center of the tumor which were not visible in the later phase due to die
leakage. Instead, OCT-A showed a series of vascular irregularities, namely,
dilatation and vascular tortuosity and rarefied capillaries. The deformation of
retinal vessels toward the center of tumor caused stretching of capillaries in
the circumpapillary region which was clearly visible on OCT images. This
technique also showed that the superficial retinal vessels had lost most of
their collateral branches and presented many loops. At deep plexus level, the
OCT images showed alterations of vessel size and morphology. These findings
confirm the histopathological features of the tumor reported by Gass[6].
In
conclusion, OCT-A imaging provides an accurate picture of the vascularization
of juxtapapillary hamartomas. This non-invasive technique may improve the
diagnosis and follow-up of patients affected by this benign tumor.
ACKNOWLEDGEMENTS
We thank Jean Ann Gilder (Scientific Communication srl., Naples, Italy) for
editing the manuscript.
Conflicts of Interest: Cennamo G, None; Romano MR,
None; Breve MA, None; Velotti N, None; de Crecchio G,
None; Cennamo G, None.
References
1 Albrecht E. Verh. dt. Path. Ges
1904;7:153.
2 Schachat AP, Shields JA, Fine SL, Sanborn GE, Weingeist TA, Valenzuela
RE, Brucker AJ. Combined hamartomas of the retina and retinal pigment
epithelium. Ophthalmology 1984;91:1609-1615.
[CrossRef]
3 Arepalli S, Pellegrini M, Ferenczy SR, Shields CL. Combined hamartoma
of the retina and retinal pigment epithelium: findings on enhanced depth
imaging optical coherence tomography in eight eyes. Retina 2014;34(11):2202-2207. [CrossRef] [PubMed]
4 Chhablani J, Rao HB, Begum VU, Jonnadulla GB, Goud A, Barteselli G.
Retinal ganglion cells thinning in eyes with non-proliferative idiopathic
macular telangiectasia type 2A. Invest
Ophthalmol Vis Sci 2015;56(2):1416-1422. [CrossRef] [PubMed]
5 Spaide RF, Klancnik JM Jr, Cooney MJ. Retinal vascular layers imaged
by fluorescein angiography and optical coherence tomography angiography. JAMA Ophthalmol 2015;133(1):45-50. [CrossRef] [PubMed]
6 Gass JD. An unusual hamartoma of
the pigment epithelium and retina simulating choroidal melanoma and
retinoblastoma. Trans Am Ophthalmol Soc 1973;71:175-183.
7 Mele A, Cennamo G, Sorrentino V, Capobianco S. Fluoroangiographic and
echographic study on a juxtapapillary hamartoma of the retinal pigment
epithelium. Ophthalmologica 1984;189(4):180-185.
[CrossRef]