Table 1 Characteristics of children with ocular trauman(%)
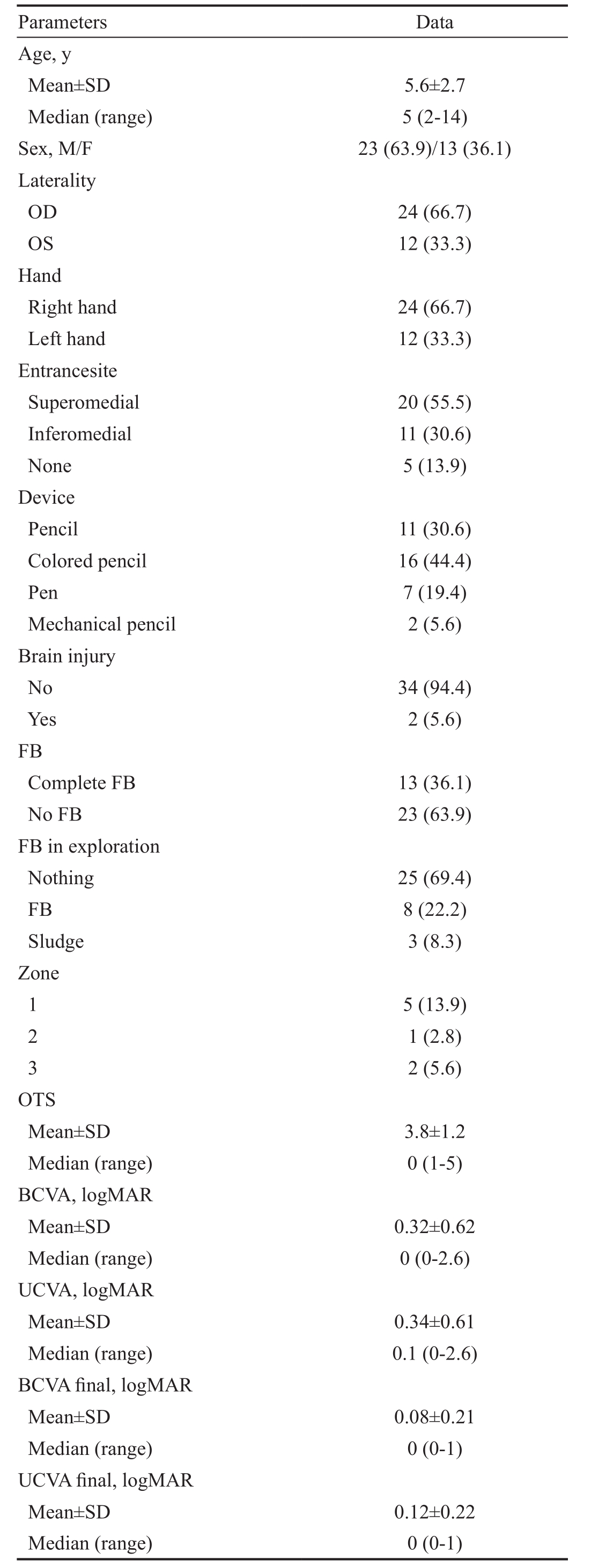
BCVA: Best corrected visual acuity; UCVA: Uncorrected visual acuity; FB: Foreign body; OD: Right eye; OS: Left eye.
Seyed Ali Tabatabaei, Mohammad Soleimani, Morteza Naderan, Aliasghar Ahmadraji, Mohammad Bagher Rajabi, Hajar Jafari, Mona Safizade
Department of Ophthalmology, Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran 1336616351, Iran
Abstract
●AlM:To determine characteristic features of ocular trauma resulted from self-trauma by writing instruments among pediatric population.
●METHODS:Thirty-six children who suffered from selfinflicted ocular trauma with a writing instrument were included in this prospective cross-sectional study.
●RESULTS:The mean age was 5.6±2.7y with male:female ratio of 1.77. The right eye was involved two times more than the left eye. The superomedial (55.5%) and inferomedial (30.6%) quadrants were the most common sites of injury. The leading culprit was colored pencils(44.4%). During surgical exploration, no foreign body (FB)was found in 25 (69.4%) patients while an FB was found in 11 (30.5%) patients. Brain injury was present in two patients (5.6%) and only in superomedial quadrant injuries.Zone 1 was the most common site for ocular trauma associated with penetrating injury. The mean ocular trauma score (OTS) in penetrating injuries was 3.8±1.2.The best corrected visual acuity (BCVA) was 0.3±0.6 upon admittance and 0.08±0.21 after one year. The final BCVA was significantly correlated with the entrance site, better final BCVA was found in nasal entrance site (P<0.05).
●CONCLUSlON:The ophthalmologists should keep a high index of suspicion to rule out penetrating eye injuries related to writing instruments in a young uncooperative child. Brain injury is a life-threatening event that should be ruled out by appropriate imaging. Medial canthal area as the most common site needs an especial attention in writing instrument injuries.
●KEYWORDS:pencil; pediatric; children; trauma; ocular
The occurrence of the eye injury represents a grave condition,especially if the inflicted eye is a child’s eye. With about a third of eye injuries affecting children, traumatic eye damage is a leading cause of monocular blindness globally[1-2]. The burden of penetrating eye injuries is significant in terms of both individual consequences and medical resources[3-4].
Although many of the eye injuries could be controlled by appropriate environmental safety measures, their occurrence is seldom predictable especially in the pediatric age group and seldom could be controlled when the culprit is a writing instrument. The challenges pertaining to such an event, either by the child or the caregiver, may prohibit the ophthalmologist to consider detailed and complete examination upon admittance. The condition would become worse in cases of a neglected retained foreign body (FB)[5-7].
The main purpose of the current study was to define characteristics of pediatric patients suffered from ocular injury with writing instruments by themselves from epidemiological,ophthalmological, and diagnostic points of view.
In the prospective cross section, we registered 36 children under 15 years of age presented to Farabi Eye Hospital(Tehran, Iran) during a period of 12mo with the chief complaint of self-inflicted ocular injuries by any kind of writing instruments. This study adhered to the guidelines of the Declaration of Helsinki and Ocular Trauma and Emergency Unit Review Board in Farabi Eye Hospital approved the study.Patients with penetrating injuries, suspicious to retained FB and having facial or palpebral laceration, underwent surgical exploration and primary repair with meticulous exploration for a remnant FB. The best corrected visual acuity (BCVA) was calculated in the logMAR unit. There was not any financial support to declare. All legal guardians/parents consented to participate in the study.
Statistical AnalysisKolmogrov-Smirnov test and Q-Q plot were used to evaluate the normal distribution of data. To present data we used mean, standard deviation, median and range. To compare the results before and after intervention,we used the Wilcoxon signed-rank test. To compare the visual acuity between groups we used Mann-Whitney and Kruskall-Wallis test, whenever appropriate. Comparison of other variables between penetrating injuries and non-penetrating injuries also performed byt-test, Mann-WhitneyUtest and Fisher’s exact test. All statistical analysis performed by SPSS(IBM Corp. Released 2016. IBM SPSS Statistics for Windows,Version 24.0. Armonk, NY: IBM Corp.).Pvalue less than 0.05 considered statistically significant.
Table 1 represented the main findings of our study. To summarize,the age of participants ranged from 2 to 14y with a mean age of 5.6±2.7y. Males were about twice as common as females(M/F ratio: 1.77). Not unexpectedly, the right-handed patients were twice as many as left-handed patients while the right eye was twice as much as the left eye (Table 1).
The most frequent sites of trauma were in the nasal half of the eye (85%), with superomedial (55.5%) and inferomedial(30.6%) quadrants of orbital area (including the eye) being the most common site. Interestingly, no case in superomedial quadrant was associated with a globe penetrating injury (Table 2).Colored pencil was the leading cause of damage (44.4%) with the least culprit being pens (19.4%). Brain injury was present in two patients (5.6%) and only in superomedial quadrant.
According to slit lamp examination at presentation, no FB was detected in 23 (63.9%) patients whereas an obvious FB was noticed in 13 (36.1%) patients. During surgical exploration,no FB was found in 25 (69.4%) patients while a FB was found in 11 cases (30.5%) (all were colored pencils), none of them was not intraocular. Interestingly, a sludge remnant (an FB but not formed) was present in 3 (8.3%) patients (all were colored pencils) (Figure 1).
The site of injury in cases of penetrating injuries, has been demonstrated in one of the 3 zones as depicted in Table 1[8-9].Most of them were in Zone 1. (Zone 1, wound involves only cornea. Zone 2, wound extends into anterior 5 mm of sclera.Zone 3, wound involves sclera extending more than 5 mm of the limbus.) The mean ocular trauma score (OTS) was 3.8±1.2 in penetrating injuries (Table 3).
Excluding seven patients aged three or less, we recorded visual acuity for the remaining 29 patients. The BCVA was 0.3±0.6 before exploration. The final BCVA was recorded 0.08±0.21. The final BCVA was significantly correlated with the entrance site (P<0.05). Actually, if the entrance site was in the nasal part, the BCVA was recorded higher. The BCVA was not correlated with gender, the eye involved, or the type of the writing instrument. It was also not correlated with the detection of the FB either before or during exploration. As expected, final BCVA was significantly worse in patients with penetrating injury (Table 4).
Table 1 Characteristics of children with ocular trauman(%)
BCVA: Best corrected visual acuity; UCVA: Uncorrected visual acuity; FB: Foreign body; OD: Right eye; OS: Left eye.
Table 2 Comparison of penetrating injury between different variables of the studyn(%)
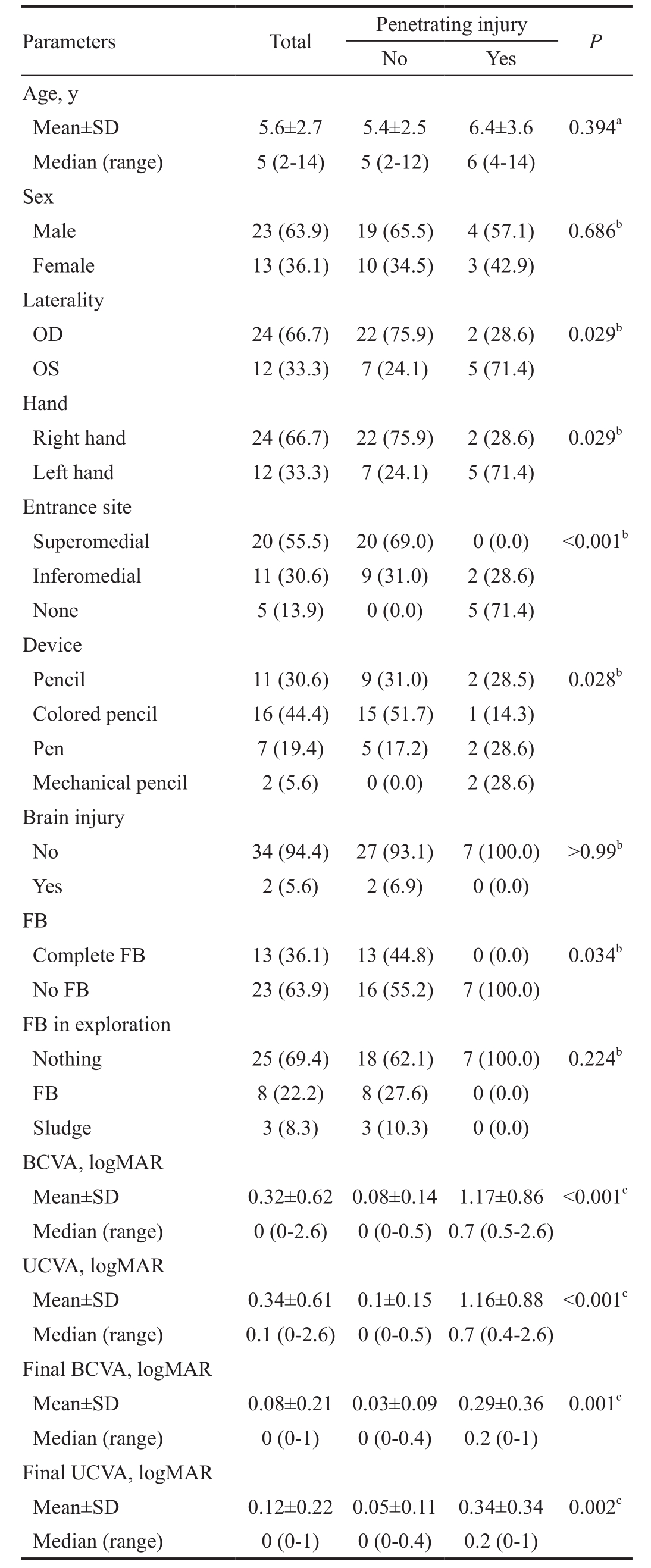
BCVA: Best corrected visual acuity; UCVA: Uncorrected visual acuity; FB: Foreign body;aBased ont-test;bBased on Fisher’s exact test;cBased on Mann-WhitneyUtest.
Ocular trauma and especially penetrating eye injuries are an ominous occurrence for both the patient and the ophthalmologist.The situation is more complicated if the patient’s condition prohibits proper and reliable history taking and primary examination, as is usually the case with pediatric population.In fact, there are astonishing reports of intraocular FB that have been diagnosed only after remote and extensive workups[5].
In this study, we reported a common identical ocular traumai.e.self-inflicted ocular trauma by a writing instrument in pediatric population.
In our study, we focused on the pediatric population whose risk of ocular trauma with writing instruments is higher in comparison to adults[2-3]. We found that black and colored pencils were the leading cause of damage which points to the importance of supervising young children during entertaining occasions. Interestingly, boys outnumbered girls in our study,as the same result reported by other investigators in other ocular traumas[10-11].
We also found the superomedial quadrant as the most common site of penetrance which is usually covered by the upper lid and may be missed or ignored if not contemplated. It may be related to the sliding the tip of the insulting device to medial canthal area. We recommend examination under anesthesia if any doubt about the examination findings in the emergency room persists.
Less than one third of our patients were found to have retained FB intraoperatively whose preliminary examination failed to demonstrate presence of such foreign materials, reflecting the importance of imaging in such cases.
The usual imaging modalities available are plain radiographs,computed tomography (CT), ultrasound, and magnetic resonance imaging (MRI). The plain films are usually discarded primarily by almost all practitioners due to their lack of precision and difficult interpretation[12]. CT is usually considered the first choice for emergent evaluation of orbital trauma, however, there are some limitations to its routine use in the setting of a penetrating injury with writing instruments.First, the major sufferers are pediatric population. The radiation associated with CT scanning and the fear of mutagenesis are drawbacks to its application especially in the very young children and especially if the history is not straightforward or the preliminary examination is not remarkable. Second, not all FB are easily detected by an unexperienced eye in the CT[13-15].In fact, the densities of various FB, represented by Hounsfield unit (HU) could be quite misleading even for an experienced practitioner. Pencils are made of wooden rod encasing a core mixture of graphite and clay. The dry wooden part is seen as a low density lesion with HU as low as -650, that may be incorrectly attributed to air, while the graphite is a denser structure with HU close to soft tissue and may be erroneously related to blood[16]. On the other hand, the distinction is notalways clear-cut because the various combination of graphite with clay or with lead containing pigments admixed as to produce color pencils may affect the density in CT scans leading to misinterpretation. Another interesting and unique outcome of the study, was the sludge during operations in colored pencils. It alerts that in some cases despite the presence of FB in orbital imaging, we could not find a formed FB and especially in red colored pencils, it necessitates excessive care,because it may be mistaken as blood. Actually colored pencils have wax liked and pigment cores that may dissolve during the presence in the body.

Figure 1 A 4-year-old boy was referred with a complaint of red colored tear
His parents mentioned a history of ocular trauma by a red pencil 3wk ago that was neglected at that time (A, B). Orbital CT scan showed retained foreign body in medial canthal area (C, D). However,during exploration, the entrance site was found to be in the caruncle, lacrimal sac was traumatized and only a sludge of red colored material was found. The patient underwent silicone intubation.
Table 3 Descriptive data of patients with penetrating injury
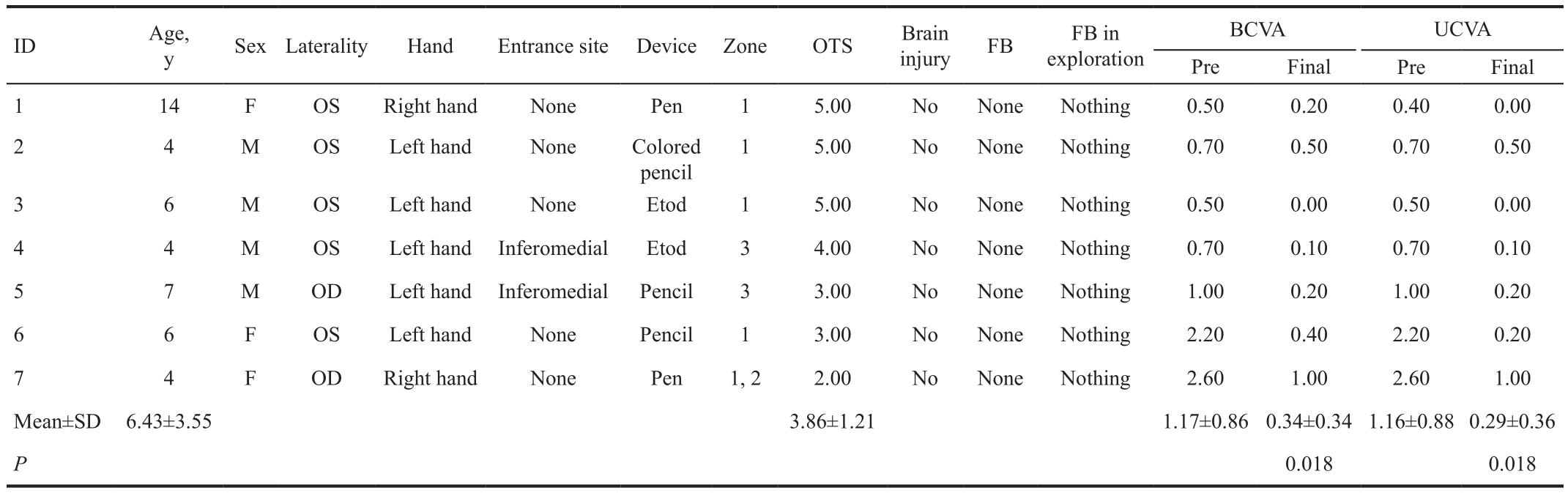
Based on Wilcoxon Signed rank test. BCVA: Best corrected visual acuity; UCVA: Uncorrected visual acuity; FB: Foreign body.
Despite effective determination of FB by ultrasound, its use is hindered in emergency settings. First, it is plagued if the FB is surrounded by air; second, it requires a cooperative patient;and the last but not the least, it is highly operator dependent.
Although MRI is considered by some authorities as a useful tool for detecting non-metallic FB, which appear as hypointense lesions, the expense, duration, and limited availability ought to be considered as drawbacks to its routine application.On the other hand, any doubt concerning the presence of a metallic FB should be ruled out by CT scan beforehand. We believe that MRI should be kept for those with proper clinical suspicion whose CT has been negative[17-18].
The OTS is a prognostic tool devised for evaluation of both open and closed globe injuries. It is used to predict the visual outcome six months after an eye injury: the higher the score,the better the prognosis[19-20]. Although some authors have proposed modifications in pediatric population considering the adverse effects of deprivation amblyopia and more aggressive healing response in children following ocular surgery[21-23], we adopted the still widely accepted adult model in our study due to its ease of application and the familiarity of our attending physicians[24]. However, the number of penetrating injuries was too law. Table 3 shows the detailed list of OTS and involved zones in penetrating injuries.
The ubiquitous presence and accessibility of writing devices even for very young children, the size, and the nature of their function necessitate more care by the parents. Although it is logical to manufacture any instrument according to some kind of safety guidelines, it has been barely tried to devise such plans for writing instruments because they are publicly viewed as ordinary harmless devices. In other words, many of the injuries related to writing instruments inflict those who are entitled to use them, namely preschool and school aged children. The ophthalmologists should keep a high index of suspicion to rule out penetrating eye injuries related to writing instruments in a young uncooperative child. Brain injury is a life threatening event that should be ruled out by appropriate imaging. Medial canthal area as the most common site needs an especial attention in writing instrument injuries.
Table 4 Comparison of final BCVA and final UCVA between different subgroups of the study
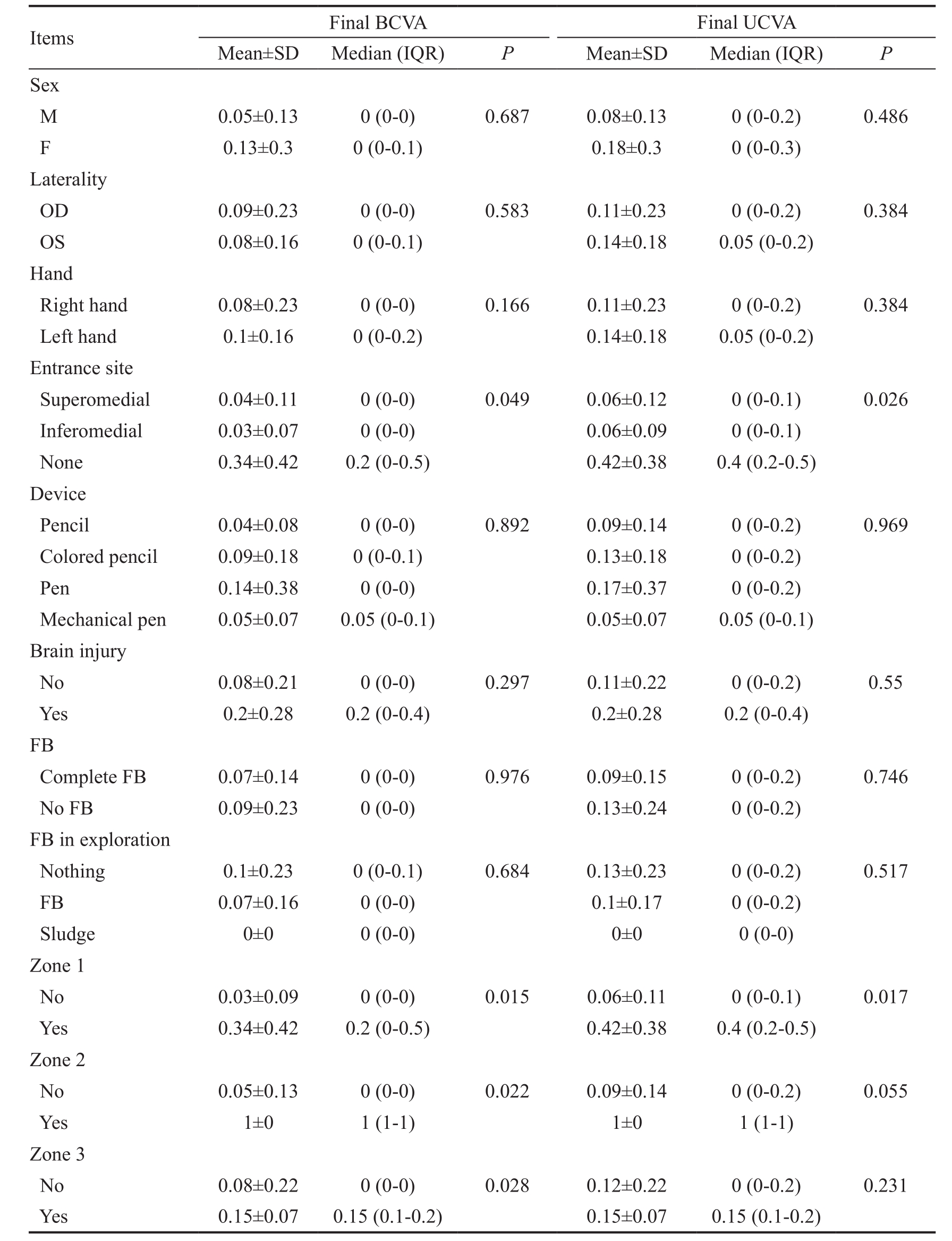
BCVA: Best corrected visual acuity; UCVA: Uncorrected visual acuity; FB: Foreign body. Based on Mann-Whitney or Kruskall-Wallis status, whenever appropriate.
We should thank Juliet Jahani and Leila Feizinia, who intimately helped us in data gathering.
Conflicts of Interest:Tabatabaei SA, None; Soleimani M,None; Naderan M, None; Ahmadraji A, None; Rajabi MB,None; Jafari H, None; Safizade M, None.
REFERENCES
1 Keel S, Xie J, Foreman J, Taylor HR, Dirani M. The prevalence of vision loss due to ocular trauma in the Australian National Eye Health Survey.Injury2017;48(11):2466-2469.
2 Sharma B, Singh S, Kumar K, Dubey A, Ahirwar K. Epidemiology,clinical profile and factors, predicting final visual outcome of pediatric ocular trauma in a tertiary eye care center of central India.Indian J Ophthalmol2017;65(11):1192-1197.
3 Cao H, Li L, Zhang M, Li H. Epidemiology of pediatric ocular trauma in the Chaoshan region, China, 2001-2010.PLoS One2013;8(4):e60844.
4 Kuhn F. Ocular traumatology: from military medicine to individual brilliance.Graefes Arch Clin Exp Ophthalmol2013;251(3):627-628.
5 Ahmad SS, Ghani SA, Peng KS, Sellamuthu P. 5-year-old girl with left upper eyelid swelling.Digit J Ophthalmol2012;18(4):15-17.
6 Yeniad B, Beginoglu M, Ozgun C. Missed intraocular foreign body masquerading as intraocular inflammation: two cases.Int Ophthalmol2010;30(6):713-716.
7 John SS, Rehman TA, John D, Raju RS. Missed diagnosis of a wooden intra-orbital foreign body.Indian J Ophthalmol2008;56(4):322-324.
8 Szijártó Z, Gaál V, Kovács B, Kuhn F. Prognosis of penetrating eye injuries with posterior segment intraocular foreign body.Graefes Arch Clin Exp Ophthalmol2008;246(1):161-165.
9 Maneschg OA, Resch M, Papp A, Németh J. Prognostic factors and visual outcome for open globe injuries with intraocular foreign bodies.Klin Monbl Augenheilkd2011;228(9):801-807.
10 Tok O, Tok L, Ozkaya D, Eraslan E, Ornek F, Bardak Y. Epidemiological characteristics and visual outcome after open globe injuries in children.J AAPOS2011;15(6):556-561.
11 Lee CH, Lee L, Kao LY, Lin KK, Yang ML. Prognostic indicators of open globe injuries in children.Am J Emerg Med2009;27(5):530-535.
12 Betts T, Ahmed S, Maguire S, Watts P. Characteristics of nonvitreoretinal ocular injury in child maltreatment: a systematic review.Eye(Lond)2017;31(8):1146-1154.
13 Patel SN, Langer PD, Zarbin MA, Bhagat N. Diagnostic value of clinical examination and radiographic imaging in identification of intraocular Foreign bodies in open globe injury.Eur J Ophthalmol2012;22(2):259-268.
14 Cho WK, Ko AC, Eatamadi H, Al-Ali A, Abboud JP, Kikkawa DO,Korn BS. Orbital and orbitocranial trauma from pencil fragments: role of timely diagnosis and management.Am J Ophthalmol2017;180:46-54.
15 Andreoli MT, Yiu G, Hart L, Andreoli CM. B-scan ultrasonography following open globe repair.Eye (Lond)2014;28(4):381-385.
16 Li J, Zhou LP, Jin J, Yuan HF. Clinical diagnosis and treatment of intraorbital wooden foreign bodies.Chin J Traumatol2016;19(6):322-325.
17 Zhou L, Li SY, Cui JP, Zhang ZY, Guan LN. Analysis of missed diagnosis of orbital foreign bodies.Exp Ther Med2017;13(4):1275-1278.
18 Modjtahedi BS, Rong A, Bobinski M, McGahan J, Morse LS. Imaging characteristics of intraocular foreign bodies: a comparative study of plain film X-ray, computed tomography, ultrasound, and magnetic resonance imaging.Retina2015;35(1):95-104.
19 Uysal Y, Mutlu FM, Sobaci G. Ocular trauma score in chilhood openglobe injuries.J Trauma2008;65(6):1284-1286.
20 Cillino S, Casuccio A, Di Pace F, Pillitteri F, Cillino G. A five-year retrospective study of the epidemiological characteristics and visual outcomes of patients hospitalized for ocular trauma in a Mediterranean area.BMC Ophthalmol2008;8:6.
21 Acar U, Tok OY, Acar DE, Burcu A, Ornek F. A new ocular trauma score in pediatric penetrating eye injuries.Eye(Lond)2011;25(3):370-374.
22 Kadappu S, Silveira S, Martin F. Aetiology and outcome of open and closed globe eye injuries in children.Clin Exp Ophthalmol2013;41(5):427-434.
23 Uysal Y, Mutlu FM, Sobaci G. Ocular trauma score in childhood openglobe injuries.J Trauma2008;65(6):1284-1286.
24 Li X, Zarbin MA, Bhagat N. Pediatric open globe injury: a review of the literature.J Emerg Trauma Shock2015;8(4):216-223.
Citation:Tabatabaei SA, Soleimani M, Naderan M, Ahmadraji A, Rajabi MB, Jafari H, Safizade M. A survey of incidental ocular trauma by pencil and pen.Int J Ophthalmol2018;11(10):1668-1673
DOl:10.18240/ijo.2018.10.15
Accepted:2018-05-17
Received:2018-02-07
Correspondence to:Mohammad Soleimani. Eye Research Center, Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran 1336616351, Iran. Soleimani_md@yahoo.com