Association between tear film break up time and blink interval in visual display terminal users
Miki Uchino1, Motoko Kawashima1, Yuichi Uchino1, Kazuo Tsubota1, Norihiko Yokoi2
1Department of Ophthalmology, Keio University School of Medicine, Tokyo 160-8582, Japan
2Department of Ophthalmology, Kyoto Prefectural University School of Medicine, Kyoto 602-8566, Japan
Abstract
●AlM:To investigate the association between tear film break up time (TBUT) and blinking interval in visual display terminal (VDT) users.
●METHODS:Nine hundred and thirty VDT users underwent dry eye testing, and functional visual acuity(FVA) test. The blinking interval during FVA was compared with TBUT. Subjects with longer blinking interval than TBUT were considered as unstable tear film. Logistic regression analysis revealed the risk factors for unstable tear group.
●RESULTS:Among 930 workers, 858 subjects (92.3%)participated in this study. Almost 80% of the subjects were categorized into the unstable tear group. Unstable tear group has significantly lower Schirmer values and TBUT (17.5±11.6vs21.1±11.5 mm, 3.7±2.6vs5.7±2.7s, bothP<0.001). There were no significant differences in epithelial staining or severity of symptoms. Logistic regression showed that over 40y was a risk for being unstable tear group [odds ratio (OR)=1.53; 95% confidence interval(Cl)=1.06-2.20]. Contact lens use was protective factor for being in the unstable tear group (OR=0.37; 95%Cl=0.26-0.53).
●CONCLUSlON:Subjects with shorter TBUT than blinking interval are prevalent among VDT users. Subjects over the age of 40 shows an increased risk for unstable tear film.
●KEYWORDS:dry eye disease; blink interval; tear film break up time; visual display terminal use
INTRODUCTION
Dry eye disease (DED) is one of the most prevalent diseases that lead patients to seek eye care[1]and this condition is especially common among visual display terminal (VDT) users, who often also suffer from severe eye fatigue[2]. Recently, the Asia Dry Eye Society revised the dry eye diagnostic criteria and updated the definition of DED as follows: “dry eye is a multifactorial disease characterized by unstable tear film causing a variety of symptoms and/or visual impairment, potentially accompanied by ocular surface damage.” This new definition stresses stability of the tear film as well as the importance of visual impairment, highlighting the essential role of tear film break up time (TBUT). A TBUT of less than or equal to 5s, considered to be decreased, is now categorized as a criterion for DED by this new definition[3].
Recent findings in the field of epidemiology have revealed that short TBUT-type dry eye, which indicates unstable tear film, is more prevalent than other types of dry eye[4].
Our group previously reported that, no or minor epithelial damage, subjective symptoms in short TBUT-type dry eye patients were almost as severe as those in definite DED patients[5].
Because patients with short TBUT-type dry eye have normal tear production and almost no vital staining, it is unclear why these patients suffer from symptoms similar to those seen in tear deficient-type DED patients who also have ocular surface damage. However, it is well known that ocular surface health and stable tear production requires frequent enough blinking in order to provide moisture and to renew the tear film. Blinking is an important compensation method for subjects who have unstable tear production, and blink rate has been reported to increase significantly in dry eye patients[6]. Blinking appears to be determined by local ocular surface conditions in conjunction with psychological and environmental factors[6]. Because blinking renews the tear film and covers the cornea, we sought to reveal the relationship between TBUT and blinking interval. We thus measured the number of blinks during the functional visual acuity (FVA) test and calculated the blinking interval from these data. We then compared blinking interval with TBUT, and we classified subjects who showed a longer blinking interval than TBUT as belonging to the “unstable tear group” because the region of the cornea where the tear film is broken is not covered with tear film. The aim of this study was to reveal the prevalence and risk factors for showing unstable tear film using a multivariable logistic regression model.
SUBJECTS AND METHODS
Study PopulationUnder the supervision of the Japanese Dry Eye Society, we conducted a large-scale epidemiologic study of office workers who use VDTs in Japan. The study was a questionnaire-based assessment of DED symptoms combined with dry eye examinations carried out by dry eye specialists investigating the epidemiology, risk factors, and pathology of DED. This study was conducted in Higashi-yodogawaku and Moriguchi town, Osaka, Japan, between 2012 and 2013.Participants in this study were employed using VDTs at either a pharmaceutical company (Santen Pharmaceutical Co. the Osaka study[7]) or at the AVC Networks Company (Panasonic Corporation, Moriguchi Study[8]).
We enrolled employees at the two companies who were willing to participate in this study. Among the 930 workers who participated in the ophthalmological tests, we randomly selected 858 (92.3%) for a detailed dry eye examination which included FVA. Subjects who reported a history of refractive surgery were excluded from the study protocol. This crosssectional research followed the tenets of the Declaration of Helsinki. Further, the Institutional Review Board of Ryogoku Eye Clinic in Tokyo, Japan prospectively approved the protocol. Written informed consent was obtained from all participants.
Dry Eye Symptom QuestionnaireWe administered a dry eye questionnaire that is widely used in Japan[9]. Briefly, the questionnaire includes 12 questions pertaining to the diagnostic symptoms of DED. The possible answers to questions regarding the frequency of DED symptoms are “constantly”,“often”, “sometimes” and “never”. The degree of DED symptoms can be reported as “very intense”, “intense”, “some”and “none”.
Information on age, sex, and smoking status (current smoker or no) was also obtained. For the detail of smoking status,if current smoking was positive, then we further asked the amount of smoking per day, and smoking years). Based on our previous studies, we defined the duration of VDT use as none to over 10h in 1h categories, and we also assessed contact lens(CL) use (yes or no)[1,10]. A history of hypertension or diabetes mellitus (DM) was determined by asking participants whether their physician had ever told them of these conditions. We defined systemic medication use as medication prescribed only by a doctor as opposed to over-the-counter supplements. We also asked the subjects whether they feel stress in their daily life (yes or no).
Tear Function and Ocular Surface EvaluationOphthalmic examinations were performed by DED specialists and included an assessment of conjunctival and corneal vital staining with lissamine green and fluorescein as well as TBUT measurement and administration of the Schirmer test. Those DED specialists were ophthalmologists who belong to the Japanese Dry Eye Society. Tear stability was assessed by the standard TBUT measurement before evaluating keratoconjunctival epithelial damage. To determine TBUT, fluorescein vital staining was administered, and subjects were requested to blink 3 times to ensure adequate mixing of the fluorescein dye with tears.The time interval between the last complete blink and the appearance of the first corneal dark spot was measured by a stopwatch, and the mean of 3 measurements was regarded as the TBUT value. Corneal and conjunctival epithelial damage were separately assessed by 2 µL of preservativefree 1% lissamine green and 1% sodium fluorescein,administered by micropipette. The eye was categorized into 3 equal compartments representing temporal conjunctiva,nasal conjunctiva, and cornea. All three parts were separately scored with the maximum staining score for 3 points. Overall epithelial staining was scored according to severity on a scale of 0-9 points[11]. Following all other examinations, the Schirmer test was administered without anesthesia using a sterilized Schirmer strip (Whatman No.41; Showa, Tokyo, Japan). We allowed a 10min interval before administering the Schirmer test in order to avoid the influence of conjunctivocorneal staining on the test results. For minimizing the measuring variety of Schirmer methods, only one examiner proceeded all the Schirmer testing. In order to avoid the influence of CL,all subjects had removed their CL at least one day before the examinations.
Functional Visual Acuity Measurement SystemAn FVA measurement system (Kowa, Aichi, Japan) was used to examine the change in continuous visual acuity over time.FVA was measured for 60s with daily vision correction without topical anaesthesia[12-13]. The FVA measurement device automatically measured blink frequency. The FVA test was carried out before all tear function examinations. In order to avoid bias, the subjects were not informed that blinks would be counted during the FVA test.
Blink IntervalBlinking interval was calculated by dividing 60s by the number of blinks counted in one minute during the FVA test. The subject who showed a longer blinking interval than TBUT was considered to have broken tear film and were categorized as belonging to the unstable tear group. Subjects whose cornea was always covered with tear film during the FVA test were categorized as belonging to the stable tear group.
Statistical AnalysisWe used Fisher’s exact test,U-tests, andt-tests to compare parameters between subjects with unstable tear group and those with stable tear group. Using a logistic regression model, we calculated the odds ratios (ORs) and 95% confidence intervals (CIs) of the unstable tear group for sex, age, smoking status, VDT use, CL use, and stress.First, we carried out univariate analyses to determine the associations between each factor and the unstable tear group.
Table 1 Characteristics of the study populationn(%)
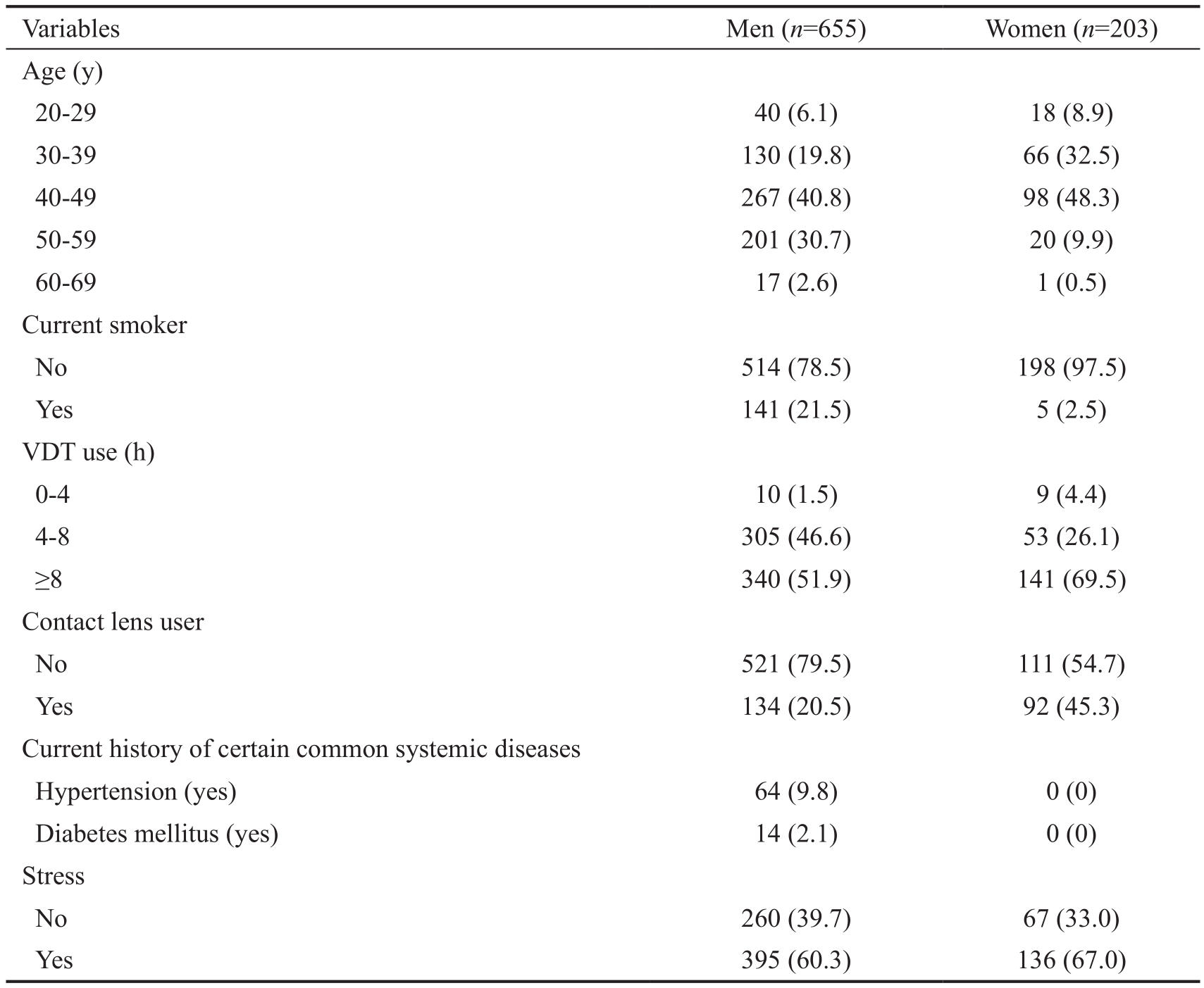
VDT: Visual display terminal.
Men (n=655) Women (n=203)Age (y)20-29 40 (6.1) 18 (8.9)30-39 130 (19.8) 66 (32.5)40-49 267 (40.8) 98 (48.3)50-59 201 (30.7) 20 (9.9)60-69 17 (2.6) 1 (0.5)Current smoker No 514 (78.5) 198 (97.5)Yes 141 (21.5) 5 (2.5)VDT use (h)0-4 10 (1.5) 9 (4.4)4-8 305 (46.6) 53 (26.1)≥8 340 (51.9) 141 (69.5)Contact lens user No 521 (79.5) 111 (54.7)Yes 134 (20.5) 92 (45.3)Current history of certain common systemic diseases Hypertension (yes) 64 (9.8) 0 (0)Diabetes mellitus (yes) 14 (2.1) 0 (0)Stress No 260 (39.7) 67 (33.0)Yes 395 (60.3) 136 (67.0)Variables
We then performed multi-adjustment for all factors identified in univariate analyses as showing aPvalue greater than 0.2.Because almost half of the subjects used VDTs more than 8h per day, we defined prolonged VDT working hours as over 8h per day in order to split the study group in roughly half by VDT use. All statistical analyses were performed using SAS software version 9.4 (SAS Inc, Cary, North Carolina, USA). APvalue of <0.05 was considered to be statistically significant.
RESULTS
Among the 930 workers in the two companies used to recruit subjects, 858 employees were randomly selected to complete this study. Of these, 655 were male (76.3%) and 203 were female (23.7%). The age of the subject group ranged between 20 and 69y (Table 1), and most of the participants were youngto-middle aged (30-49 years old accounted for 65.4% of the study population). The rate of smoking was almost 10 times higher in men than in women (21.5%vs2.5%). The duration of VDT use was relatively long: 51.9% of male participants and 69.5% of female participants reported using VDTs for over 8h per day, and only 1.5% of men and 4.4% of women reported using VDTs for less than 4h per day. The number of participants with systemic disease was low for both male and female participants. No female subjects reported any systemic disease, and the percentage of men reporting hypertension and DM was 9.8% and 2.1%, respectively. Almost two-thirds of subjects reported feeling stress in their daily life (Table 1).The stress did not show any significance between the two subgroups.
The demographic data for the unstable tear film group and the stable tear film group are shown in Table 2. Almost 80% of the participants were categorized into the unstable tear film group, and this group was significantly older than the stable tear group (P=0.001). Further, members of the unstable tear group were more likely to be men and to report shorter VDT time (P=0.001 andP=0.009, respectively). The two groups did not differ by reported existence of daily stress or by frequency or intensity of dry eye symptoms (P=0.54, 0.18, and 0.13,respectively). In the ocular findings, we found that subjects with unstable tear film showed significantly lower Schirmer values (17.5±11.6vs21.1±11.5 mm,P<0.001), shorter TBUTs(3.7±2.6vs5.7±2.7s,P<0.001), and lower blinking counts(7.6±7.0vs22.7±9.8,P<0.001). There was no significant difference in the number of epithelial staining points (P=0.081;Table 2).
Using a logistic regression model, we assessed the risk factors for being in the unstable tear group. We calculated the ORs and 95%CIs of the unstable tear group for sex, age, smoking status, VDT use, CL use, and stress. The results of the univariate and multivariate analyses are shown in Table 3.According to the multivariate-adjusted model, unstable tearfilm was significantly associated with an age of over 40 years old (OR=1.53, 95%CI=1.06-2.20,P=0.023). CL use was significantly negatively associated with belonging to the unstable tear group (OR=0.37, 95%CI=0.26-0.53,P<0.001).Although prolonged VDT hours were reported by over half of our subjects, and the OR for VDT hours was significant in univariate analysis, the association between prolonged VDT use and the risk of unstable tear group in the multivariate model was not significant after adjusting for the age, sex, VDT working hours, and CL use (OR=0.78, 95%CI=0.55-1.12,P=0.180). Additionally, men were significantly more likely to be in the unstable tear group by univariate analysis, but this relationship was not significant when the multivariate model was applied (OR=0.74, 95%CI=0.50-1.09,P=0.122). Stress was not associated with unstable tear film.
Table 2 Demographic finding between short break up time mean±SD,n(%)
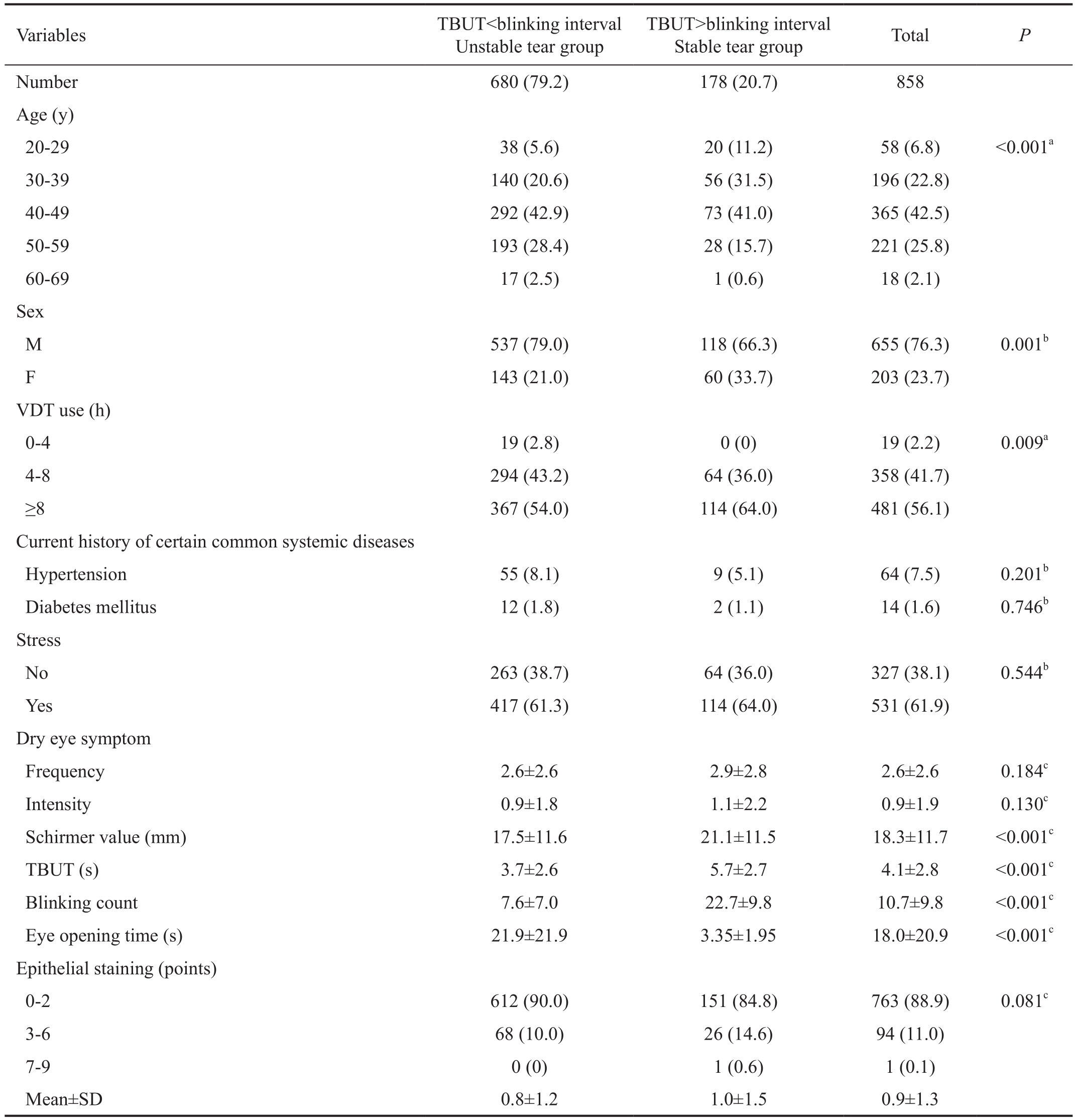
TBUT: Tear film break up time; VDT: Visual display terminal.aU-test,bFishers exact test,ct-test.
38 (5.6) 20 (11.2) 58 (6.8) <0.001a30-39 140 (20.6) 56 (31.5) 196 (22.8)40-49 292 (42.9) 73 (41.0) 365 (42.5)50-59 193 (28.4) 28 (15.7) 221 (25.8)60-69 17 (2.5) 1 (0.6) 18 (2.1)Sex M 537 (79.0) 118 (66.3) 655 (76.3) 0.001bF 143 (21.0) 60 (33.7) 203 (23.7)VDT use (h)0-4 19 (2.8) 0 (0) 19 (2.2) 0.009a4-8 294 (43.2) 64 (36.0) 358 (41.7)≥8 367 (54.0) 114 (64.0) 481 (56.1)Current history of certain common systemic diseases Hypertension 55 (8.1) 9 (5.1) 64 (7.5) 0.201bDiabetes mellitus 12 (1.8) 2 (1.1) 14 (1.6) 0.746bStress No 263 (38.7) 64 (36.0) 327 (38.1) 0.544bYes 417 (61.3) 114 (64.0) 531 (61.9)Dry eye symptom Frequency 2.6±2.6 2.9±2.8 2.6±2.6 0.184cIntensity 0.9±1.8 1.1±2.2 0.9±1.9 0.130cSchirmer value (mm) 17.5±11.6 21.1±11.5 18.3±11.7 <0.001cTBUT (s) 3.7±2.6 5.7±2.7 4.1±2.8 <0.001cBlinking count 7.6±7.0 22.7±9.8 10.7±9.8 <0.001cEye opening time (s) 21.9±21.9 3.35±1.95 18.0±20.9 <0.001cEpithelial staining (points)0-2 612 (90.0) 151 (84.8) 763 (88.9) 0.081c3-6 68 (10.0) 26 (14.6) 94 (11.0)7-9 0 (0) 1 (0.6) 1 (0.1)Mean±SD 0.8±1.2 1.0±1.5 0.9±1.3 Variables TBUT<blinking interval Unstable tear group TBUT>blinking interval Stable tear group TotalPNumber680 (79.2) 178 (20.7) 858 Age (y)20-29
DISCUSSION
It is well known that ocular surface health and stable tear film require frequent blinking in order to induce tears and thus renew the tear film. A shorter TBUT has been reported to be associated with more severe DED symptoms in VDT users[5]. Although clinical observations have long suggested the importance of tear film in eye health, no previous study hassought to determine the magnitude of the association between TBUT and blinking interval. In addition, many studies have reported that VDT workers commonly report eye problems but no large scale study has investigated the risk factors associated with unstable tear film and blinking[14]. This large cross-sectional study is the first to examine the prevalence of unstable tear film and to evaluate potential risk factors in office workers who use VDTs.
Table 3 Association between demographic, lifestyle, and unstable tear group
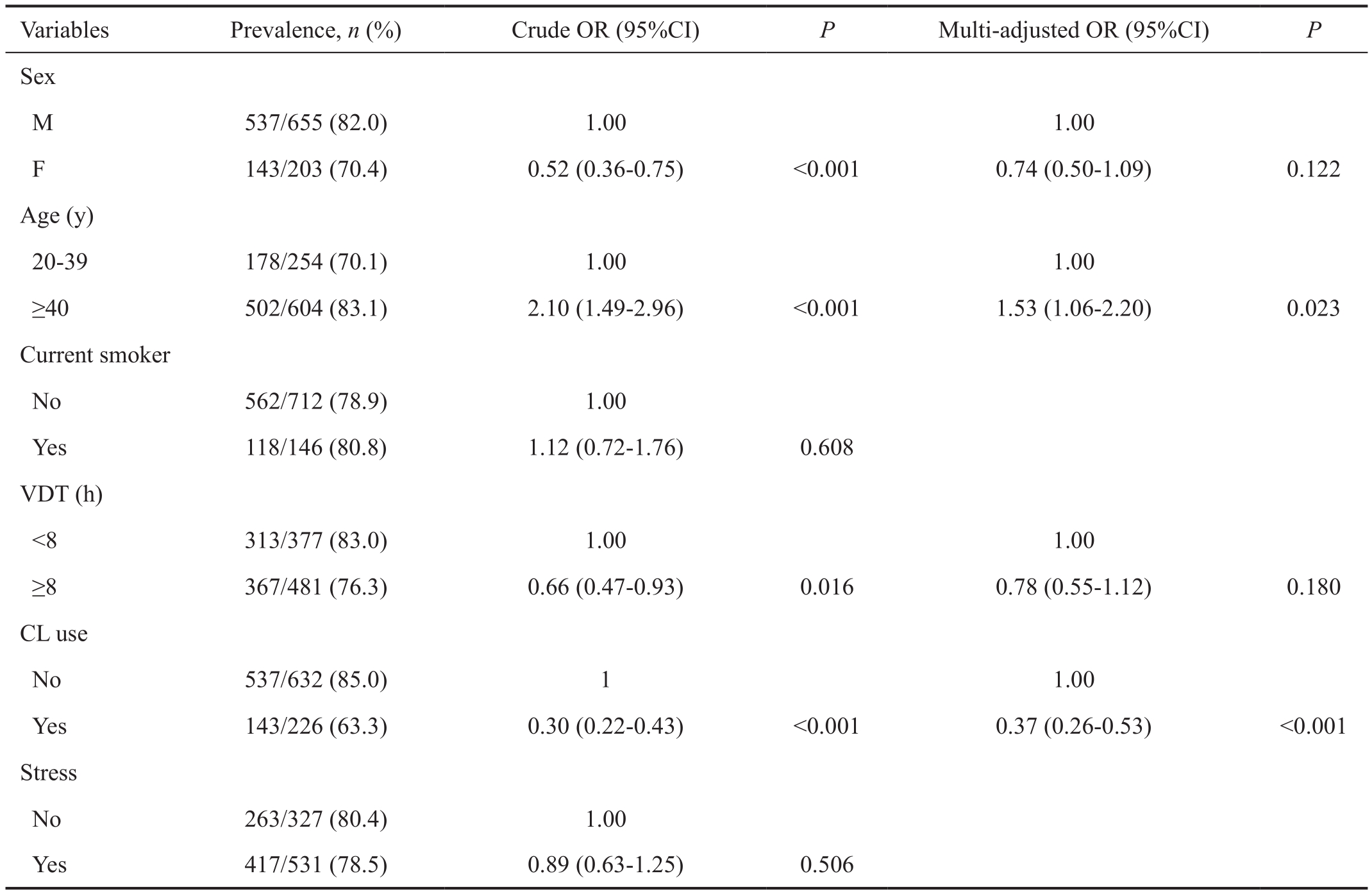
VDT: Visual display terminal; CL: Contact lens. Adjusted for age and all of the associated factors identified in the univariate analyses (P<0.2).
Variables Prevalence,n(%) Crude OR (95%CI)PMulti-adjusted OR (95%CI)PSex M 537/655 (82.0) 1.00 1.00 F 143/203 (70.4) 0.52 (0.36-0.75) <0.001 0.74 (0.50-1.09) 0.122 Age (y)20-39 178/254 (70.1) 1.00 1.00≥40 502/604 (83.1) 2.10 (1.49-2.96) <0.001 1.53 (1.06-2.20) 0.023 Current smoker No 562/712 (78.9) 1.00 Yes 118/146 (80.8) 1.12 (0.72-1.76) 0.608 VDT (h)<8 313/377 (83.0) 1.00 1.00≥8 367/481 (76.3) 0.66 (0.47-0.93) 0.016 0.78 (0.55-1.12) 0.180 CL use No 537/632 (85.0) 1 1.00 Yes 143/226 (63.3) 0.30 (0.22-0.43) <0.001 0.37 (0.26-0.53) <0.001 Stress No 263/327 (80.4) 1.00 Yes 417/531 (78.5) 0.89 (0.63-1.25) 0.506
In the current study, 79.2% of subjects showed a longer blinking interval than TBUT and were thus considered to have unstable tear film. This high percentage was somewhat surprising given the relatively young age of the study population. We found that unstable tear film was significantly more prevalent in men (82.0%) and in subjects who were over the age of 40 (bothP<0.001). Men showed a higher prevalence of being in the unstable tear group compared with women, indicating that men may have a better ability to keep their eyes open after the tear film has been broken. The gender differences in the current study therefore might be explainable by differences in the way that each gender reacts to pain.When the tear film over the cornea breaks after a time without blinking, we start to feel pain. Fillingimet al[15]reported that clinical and epidemiologic findings indicate that women are at increased risk for many chronic pain conditions and tend to report higher levels of acute procedural pain. Further, a previous Meta-analysis demonstrated the existence of sex differences in experimental pain sensitivity[16]. It is thought that such sex-related differences in pain are likely due to the interaction of biological differences between men and women(e.g.genetic or hormonal factors) with psychological and socio-cultural factors[15].
Our study also revealed that subjects who reported daily CL use were less likely to be in the unstable tear group because they frequently blinked during the FVA test. We asked CL users not to wear CL and FVA examinations were performed in the absence of CL. We hypothesized that the absence of CL might have caused subjects to blink more frequently during the FVA measurement due to stronger symptoms. As far as we know, there are many studies that have reported on the association between CL associated with ocular irritation[17-20]. Zhanget al[17]investigated ocular irritation in the presence and absence of CL wear and reported that discomfort was significantly greater during trials without CL wear, indicating that a CL may act as a barrier between the outside environment and the cornea and thus affect the sensory response to TBUT and reduce discomfort. Martín-Montañezet al[18]also investigated CL use and reported that subjects who reported more severe eye dryness also showed increased blink rates during CL wear, indicating that an increased blink rate might improve the ocular surface environmentand relieve symptoms. Another effect of CL wear on ocular health is reduced corneal nerve function. Murphyet al[19]reported that CL wear decreases corneal sensitivity, and Patelet al[20]used confocal microscopy to observe a reduction in corneal nerves in CL users. Lastly, the tendency of blinking more during CL wear might have affected the CL users in our study, even though they were not wearing CL at the time of the examinations. CL users depend on blinking to correct CL position and thus avoid reduced visual acuity[18]. Therefore,during the FVA measurements in this study, the subjects, who did not have normal protection for the ocular surface, might have increased their blinking interval to attempt to obtain better vision. Interestingly, we observed that subjects over the age of 40 had a 53% increased risk for showing an unstable tear film.
In our study, aging is founded out to be a risk factor for being unstable tears. We considered the corneal sensitivity has been playing a key role to be unstable tear. Aging is known to decrease the corneal sensitivity[18]and corneal hypoesthesia can result from both physiologic and pathologic conditions.Physiologic conditions that can lead to decreased corneal sensitivity include aging, menstrual cycle, pregnancy, and defective lid closure[21-24]. Pathologic conditions that can lead to decreased corneal sensitivity include diabetes, myasthenia gravis, leprosy, chronic inflammation, infection, corneal dystrophies, keratoconus, and trachoma[25-28]. Mirzajanet al[29]reported that subjects older than age 35 were less likely to show a corneal sensitivity of 60 mm in all corneal regions.Corneal sensitivity is one of the most important factors related to blinking. From our current study that subjects aged over 40 showed a lower blinking frequency might be supported by the reduced corneal sensitivity associated with aging.
Further, Nielsenet al[30]reported that blinking frequency has been shown to decrease in certain conditions, such as when subjects are conducting tasks with high cognitive and visual demands. These conditions are becoming more common as people work or spend their leisure time in front of VDTs. This phenomenon is not limited to the younger generation but is also seen in older subjects. The results of our study might provide a useful warning to older VDT users to increase blinking in order to obtain a stable tear film on the cornea.
This study has several limitations. First, we only asked whether subjects used CL rather than asking for information on CL type Therefore, we were not able to investigate whether any particular type of CL has a significant effect on blink rate and TBUT. Second, the subjects in our study were recruited from the workplace, and most subjects were in good health.Therefore, our study may show the healthy worker effect,and our findings may not be applicable to patients with ophthalmologic disorders such as DED.
In conclusion, our study measured both blinking frequency and TBUT and found that unstable tear film was prevalent among VDT users. Aging was found to be a significant risk factor for showing an unstable tear film, while daily CL use was observed to be significant protective factor for being stable tear film. Although further studies are needed to increase our understanding of the significance of unstable tear film, the results of this study may provide guidance for specific precautions, such as reminding workers to blink more frequently during VDT use and adopting relevant policies in the work place to prevent unstable tear film during VDT work.
ACKNOWLEDGEMENTS
This study was a collaborative investigation of the Dry Eye Society, Tokyo, Santen Pharmaceutical Co., Ltd., Osaka, and AVC Networks Company, Panasonic Corporation, Osaka,Japan. Santen, Santen Pharmaceutical Co., Ltd and AVC Networks Company provided the research facilities, and Santen Pharmaceutical Co., Ltd. assisted in the transport of equipment.
Authors’ contributions:Miki Uchino, Motoko Kawashima,Norihiko Yokoi, and Kazuo Tsubota wrote the main manuscript text. Yuichi Uchino made all the tables. All authors reviewed the manuscript.
Conflicts of Interest:Uchino M, None; Kawashima M,None; Uchino Y, None; Tsubota K, consultant and research funding received from Santen Pharmaceutical Co., Ltd.,research funding received from Kowa Company, and holds the patent rights for the method and the apparatus used for the measurement of functional visual acuity (US patent No.7470026); Yokoi N, consultant for Kissei Co., Ltd., Alcon Japan Ltd., and Rohto Co., Ltd.
REFERENCES
1 Management and therapy of dry eye disease: report of the management and therapy subcommittee of the international dry eye work shop (2007).Ocul Surf2007;5(2):163-178.
2 Uchino M, Schaumberg DA, Dogru M, Uchino Y, Fukagawa K,Shimmura S, Satoh T, Takebayashi T, Tsubota K. Prevalence of dry eye disease among Japanese visual display terminal users.Ophthalmology2008;115(11):1982-1988.
3 Tsubota K, Yokoi N, Shimazaki J, Watanabe H, Dogru M, Yamada M,Kinoshita S, Kim HM, Tchah HW, Hyon JY, Yoon KC, Seo KY, Sun X,Chen W, Liang L, Li M, Liu Z. New perspectives on dry eye definition and diagnosis: a consensus report by the Asia dry eye society.Ocul Surf2017;15(1):65-76.
4 Uchino M, Yokoi N, Uchino Y, Dogru M, Kawashima M, Komuro A, Sonomura Y, Kato H, Kinoshita S, Schaumberg DA, Tsubota K.Prevalence of dry eye disease and its risk factors in visual display terminal users: the Osaka study.Am J Ophthalmol2013;156(4):759-766.
5 Yokoi N, Uchino M, Uchino Y, Dogru M, Kawashima M, Komuro A, Sonomura Y, Kato H, Tsubota K, Kinoshita S. Importance of tear film instability in dry eye disease in office workers using visual display terminals: the Osaka study.Am J Ophthalmol2015;159(4):748-754.
6 Prause JU, Norn M. Relation between blink frequency and break-up time?Acta Ophthalmol (Copenh)1987;65(1)19-22.
7 Uchino M, Uchino Y, Kawashima M, Yokoi N, Tsubota K. What have we learned from the Osaka study?Cornea2018 Sep 6. [Epub ahead of print]
8 Kawashima M, Yamatsuji M, Yokoi N, Fukui M, Ichihashi Y, Kato H, Nishida M, Uchino M, Kinoshita S, Tsubota K. Screening of dry eye disease in visual display terminal workers during occupational health examinations: the Moriguchi study.J Occup Health2015;57(3):253-258.
9 Toda I, Fujishima H, Tsubota K. Ocular fatigue is the major symptom of dry eye.Acta Ophthalmol(Copenh)1993;71(3):347-352.
10 Uchino M, Nishiwaki Y, Michikawa T, Shirakawa K, Kuwahara E,Yamada M, Dogru M, Schaumberg DA, Kawakita T, Takebayashi T,Tsubota K. Prevalence and risk factors of dry eye disease in Japan: Koumi study.Ophthalmology2011;118(12):2361-2367.
11 van Bijsterveld OP. Diagnostic tests in the Sicca syndrome.Arch Ophthalmol1969;82(1):10-14.
12 Kaido M, Dogru M, Yamada M, Sotozono C, Kinoshita S, Shimazaki J, Tsubota K. Functional visual acuity in Stevens-Johnson syndrome.Am J Ophthalmol2006;142(6):917-922.
13 Kaido M, Dogru M, Ishida R, Tsubota K. Concept of functional visual acuity and its applications.Cornea2007;26(9 Suppl 1):S29-S35.
14 Courtin R, Pereira B, Naughton G, Chamoux A, Chiambaretta F,Lanhers C, Dutheil F. Prevalence of dry eye disease in visual display terminal workers: a systematic review and meta-analysis.BMJ Open2016;6(1):e009675
15 Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B,Riley JL 3rd. Sex, gender, and pain: a review of recent clinical and experimental findings.J Pain2009;10(5):447-485.
16 Riley JL 3rd, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex differences in the perception of noxious experimental stimuli: a metaanalysis.Pain1998;74(2-3):181-187.
17 Zhang J, Begley CG, Situ P, Simpson T, Liu H. A link between tear breakup and symptoms of ocular irritation.Ocul Surf2017;15(4):696-703.
18 Martín-Montañez V, López-de la Rosa A, López-Miguel A. Pinto-Fraga J, González-Méijome JM, González-García MJ. End-of-day dryness, corneal sensitivity and blink rate in contact lens wearers.Cont Lens Anterior Eye2015;38(3):148-151.
19 Murphy PJ, Patel S, Marshall J. The effect of long-term, daily contact lens wear on corneal sensitivity.Cornea2001;20(3):264-269.
20 Patel SV, McLaren JW, Hodge DO, Bourne WM. Confocal microscopy in vivo in corneas of long-term contact lens wearers.Invest Ophthalmol Vis Sci2002;43(4):995-1003.
21 Roszkowska AM, Colosi P, Ferreri FM, Galasso S. Age-related modifications of corneal sensitivity.Ophthalmologica2004;218(5):350-355.
22 duToit R, Vega JA, Fonn D, Simpson T. Diurnal variation of corneal sensitivity and thickness.Cornea2003;22(3):205-209.
23 Millodot M. Diurnal variation of corneal sensitivity.Br J Ophthalmol1972;56(11):844-847.
24 Millodot M. The influence of pregnancy on the sensitivity of the cornea.Br J Ophthalmol1977;61(10):646-649.
25 Schwartz DE. Corneal sensitivity in diabetics.Arch Ophthalmol1974;91(3):174-178.
26 Adatia FA, Michaeli-Cohen A, Naor J, Caffery B, Bookman A,Slomovic A. Correlation between corneal sensitivity, subjective dry eye symptoms and corneal staining in Sjögren’s syndrome.Can J Ophthalmol2004;39(7):767-771.
27 Bourcier T, Acosta MC, Borderie V, Borrás F, Gallar J, Bury T,Laroche L, Belmonte C. Decreased corneal sensitivity in patients with dry eye.Invest Ophthalmol Vis Sci2005;46(7):2341-2345.
28 Hieselaar LC, Hogeweg M, de Vries CL. Corneal sensitivity in patients with leprosy and in controls.Br J Ophthalmol1995;79(11):993-995.
29 Mirzajan A, Khezri F, Jafarzadehpur E. Karimian F, Khabazkhoob M.Normal corneal sensitivity and its changes with age in Tehran, Iran.Clin Exp Optom2015;98(1):54-57.
30 Nielsen PK, Søgaard K, Skotte J, Wolkoff P. Ocular surface area and human eye blink frequency during VDU work: the effect of monitor position and task.Eur J Appl Physiol2008;103(1):1-7.
Citation:Uchino M, Kawashima M, Uchino Y, Tsubota K, Yokoi N. Association between tear film break up time and blink interval in visual display terminal users.Int J Ophthalmol2018;11(10):1691-16397
DOl:10.18240/ijo.2018.10.18
Accepted:2018-06-11
Received:2018-03-21
Correspondence to:Miki Uchino. Department of Ophthalmology,Keio University School of Medicine, 35 Shinanomachi,Shinjuku-ku, Tokyo 160-8582, Japan. uchinomiki@keio.jp