·Brief Report·
Superficial foveal avascular zone area changes before and after idiopathic epiretinal membrane surgery
Yo Sep Yoon, Je Moon Woo, Jong Eun Woo, Jung Kee Min
Department of Ophthalmology, Ulsan University Hospital,College of Medicine, University of Ulsan, Ulsan 44033,Republic of Korea
Abstract
●To investigate the foveal morphological changes and foveal avascular zone (FAZ) area before and after epiretinal membrane (ERM) surgery. Twenty-two eyes with treatmentnaive ERM were included in this retrospective study.The central foveal thickness (CFT) and FAZ area were measuredviaswept-source optical coherence tomography(SS-OCT) and OCT angiography pre- and postoperatively.The unaffected fellow eyes were used as controls. The preoperative superficial FAZ area was significantly smaller in patients (0.08±0.04 mm2) than in controls (0.33±0.09 mm2;P<0.001). The postoperative superficial FAZ (0.12±0.06 mm2)area was significantly greater than the preoperative area(P<0.001). The preoperative superficial FAZ area was strongly negatively correlated with CFT (P<0.001,rho=-0.763).ERM induced significant foveal morphological changes and reduction of the superficial FAZ area. Foveal thickness was restored and FAZ area increased postoperatively.However, the process is rather slow and the recovery is incomplete.
●KEYWORDS:central foveal thickness; epiretinal membrane;foveal avascular zone; optical coherence tomography angiography
INTRODUCTION
The foveal avascular zone (FAZ) is a specialized region of the human retina that contains the highest cone photoreceptor density, and is entirely devoid of retinal vessels,including capillaries; thus no blood vessels cause optical interference[1-2], and the FAZ allows light sensing without any dispersion or loss. This anatomy is responsible for the depression in the center of the fovea[3]. Epiretinal membrane(ERM) is an epimacular membranous tissue, of which the development is related to proliferative disease, inflammation,uveitis, or trauma, as well as other reasons. However, the pathology is still not completely understood. ERM can lead to tangential traction, causing retinal changes, such as retinal layers thickening, surface wrinkling, and/or nerve fiber layer fibrillation, which cause decreased visual acuity (VA) and metamorphopsia. Advanced forms of ERM with decreased VA and progressive clinical symptoms can be treated with surgical procedures such as pars plana vitrectomy (PPV), ERM, and/or internal limiting membrane (ILM) peeling[4-8]. Such surgical treatment often improves VA, but clinical symptoms, like metamorphopsia, may remain.
In healthy eyes, the size of the FAZ is not expected to affect visual function[9-11], but the relationship between FAZ size and vision in retinal diseases remains speculative. Disrupted foveal development is associated with diseases such as retinopathy of prematurity[12]and albinism[13-14]. Various aspects of foveal anatomy are also altered in retinal diseases, such as diabetic retinopathy and retinal vein occlusion[15-17]. Optical coherence tomography angiography (OCTA) is a new, noninvasive method for visualizing the retinal microcirculation[16]. Therefore, in this study, we investigated the changes in central foveal thickness(CFT) and FAZ area before and after ERM surgery, and evaluated the correlation between CFT and the superficial FAZ area using both swept-source OCT (SS-OCT) and OCTA.
SUBJECTS AND METHODS
SubjectsThis study was approved by the Institutional Human Experimentation Committee Review Board of Ulsan University Hospital (UUH 2017-08-026) and was conducted in accordance with the ethical standards set forth in the 1964 Declaration of Helsinki. After a detailed explanation of this study, informed consents were obtained from all patients. In this retrospective study, 22 eyes of 22 patients with idiopathic ERM diagnosed and surgically treated were included. Only patients with ERM,predominantly of the diffuse type, were included. Preoperative SS-OCT images showed an intact photoreceptor layer without any inner segment/outer segment (IS/OS) disruption. Patients with recurrent ERM, and any history of uveitis or prior retinal detachment were excluded. Additionally, patients with severemedia opacities affecting VA and highly myopic eyes with an axial length of 26.5 mm or more were excluded. The superficial FAZ of the unaffected fellow eyes were used as controls.
Table 1 Subject baseline demographic and ocular characteristics mean±SD

ERM: Epiretinal membrane; BCVA: Best corrected visual acuity; CFT: Central foveal thickness; FAZ: Foveal avascular zone.aWilcoxon’s signed-rank test (preoperative and postoperative ERM); Mann-WhitneyUtest (bpreoperative ERMvscontrol,cpostoperative ERMvscontrol).
Characteristic ERM (preoperative) ERM (postoperative) Fellow eye (control)PaPbPcAge, y 65.0±9.5 Male/female 10/12 Postoperative time (mo) 5.8±3.2 BCVA (logMAR) 0.47±0.19 0.17±0.13 0.02±0.05 <0.001 <0.001 <0.001 CFT (µm) 482.2±57.5 359.0±38.9 251.8±34.9 <0.001 <0.001 <0.001 Superficial FAZ area (mm2) 0.08±0.04 0.12±0.06 0.33±0.09 0.002 <0.001 <0.001
Imaging ProtocolTo analyze foveal structure and thickness,we utilized an SS-OCT & OCTA system (DRI OCT-1,Atlantis; Topcon Corporation, Tokyo, Japan). The CFT was defined as the average thickness in the central circle area of nine Early Treatment Diabetic Retinopathy Study subfields.For OCTA imaging, 3×3×3 mm3macular cubes were acquired.En face images of the retinal vasculature were generated from the superficial capillary layer (SCL) and deep capillary layer(DCL), based on the automated layer segmentation. The FAZ area was defined as the area inside the central border of the capillary network. The FAZ area in the SCL was independently graded by two investigators (Yoon SY and Woo JE). The graders manually outlined the inner border of foveal capillaries in the FAZ using the OCTA embedded software, and then the FAZ area was calculated automatically.
Surgical ProcedureAll patients underwent ERM and ILM peeling using 25-gauge PPV with the EVA vitrectomy system(DORC, Zuidland, the Netherlands) with or without triamcinolone staining (40 mg/mL) and indocyanine green (1.25 mg/mL) as a negative stain. In all patients, phacoemulsification, aspiration,and intraocular lens implantation were performed at the time of vitrectomy. All surgeries were performed by a single retinal surgeon (Min JK). No intraoperative complications were noted.
Statistical AnalysesStatistical analyses were performed using SPSS statistical software (version 18 for Windows, IBM Corporation, Armonk, NY, USA). Wilcoxon’s signed-rank test was used for quantitative data analysis before and after ERM surgery. The Mann-WhitneyUtest was used for comparison of the mean changes between the two groups (preoperative subjects versus control, postoperative subjects versus control).The relationship between the superficial FAZ area and CFT within three groups was determined using Spearman’s correlation analysis. Agreement between two examiners about the measurement of the superficial FAZ area was compared using intraclass correlation coefficients (ICCs). Continuous variables are presented as mean±standard deviations (SD), and statistical significance was defined asP<0.05.
RESULTS AND DISCUSSION
The baseline demographics and ocular characteristics of the patients were summarized in Table 1. The CFT was reduced from 482.2±57.5 µm preoperatively to 359.0±38.9 µm postoperatively(P<0.001; Table 1). Repeatability of the measurements between two examiners was good for the preoperative and postoperative superficial FAZ areas (ICC=0.855 and 0.903),and excellent for the FAZ of the control (ICC=0.949).
Since OCT came into use, there have been several publications about its use in studies of the morphology of ERM[18]and functional outcomes after surgery[19-21]. Although patients with ERM can be completely asymptomatic when the membrane is thin, its progression to a thick and contractile membrane may bring about macular distortion and/or edema, thus leading metamorphopsia and reduction of central visual function.Efforts have been made to correlate retinal thickness to VA in patients with ERM. There was a strong correlation between foveal anatomic alterations and vision[21-22]. In addition,recent studies have shown that good visual outcomes after ERM peeling is dependent on an intact photoreceptor IS/OS junction, as seen in preoperative spectral-domain OCT (SD-OCT)[23-25]. There are also patients whose visual function does not improve after ERM surgery, but who show a normal appearing photoreceptor layer on SD-OCT[26]. It has been hypothesized that other factors might contribute to distorted vision and metamorphopsia after surgery. A study measuring inner retinal changes in patients with ERM showed that metamorphopsia is related to the presence of an edematous inner nuclear layer[27]. Many studies have been made to define changes in anatomic retinal structures due to ERM as predictors for visual outcome after surgery[21,23-24,27]. These previous studies have examined predominantly inner or outer retinal layer anatomical changes, but did not investigate foveal vasculature changes that can disperse the light before it reaches the photoreceptor cells. Therefore, we examined whether retinal restoration, leading to good visual function, may be dependent on the rehabilitation of FAZ and foveal contour.
Our results showed that the area of the superficial FAZ was significantly smaller preoperatively in ERM eyes than in the unaffected fellow eyes (0.08±0.04 mm2vs0.33±0.09 mm2,P<0.001; Table 1).
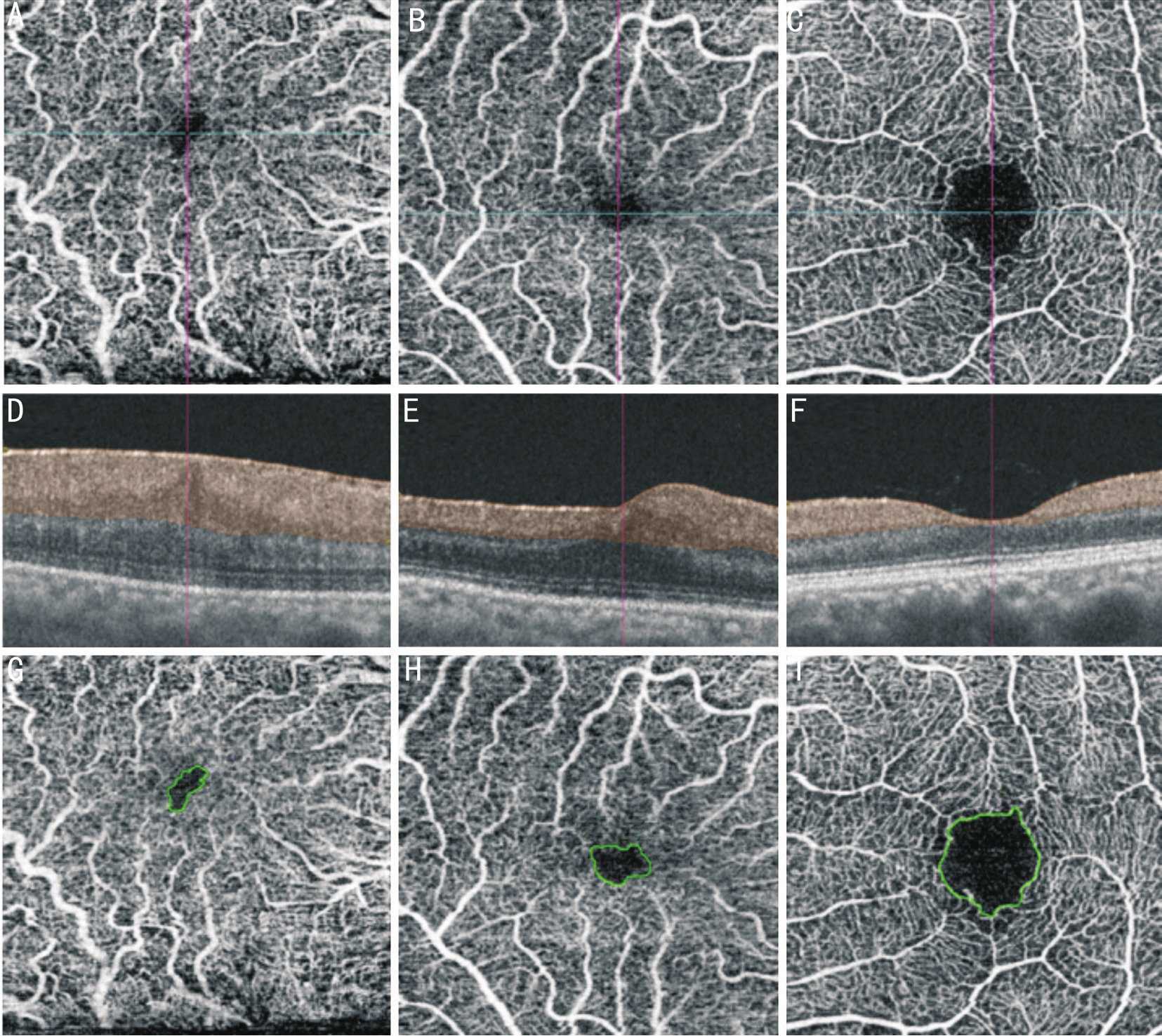
Figure 1 OCTA images of a 55 years old female patient with unilateral ERM
The SCL of the affected eye before ERM surgery (A), and of the affected right eye at postoperative 5mo (B), and of the unaffected fellow eye (C). Longitudinal scans showed the corresponding segmentation layers (D-F). The superficial FAZ was shown within the green line. Preoperative OCTA image (G) showed the distortion of the superficial retinal vasculature, the reduction and deformation of the FAZ area (0.058 mm2). Postoperative OCTA image at 5mo (H) showed the increase in the superficial FAZ area (0.108 mm2) and partial normalization of the vascular structure. The OCTA image of the SCL in the unaffected fellow eye(I). Its FAZ area measured 0.455 mm2.
The retinal changes induced by anterior-posterior force and tangential centripetal traction in the ERM may appear as irregular wrinkling, retinal layer thickening and dragging,and ectopic fovea. A shallow foveal depression, as well as a thick CFT, suggests a movement of macular tissue toward the central fovea when ERM is aggravated. The degree of foveal depression has been reported to be positively correlated with the size of the FAZ[3,10]. The centripetal movement of the foveal tissue may be the reason for the shallower foveal pit, and even foveal protrusion, and the smaller FAZ area in ERM patients.Our results support this idea, because a reduction in the FAZ area was shown when ERM had worsened and an increase in FAZ size was also shown after ERM surgery (Table 1,Figure 1). After ERM surgery, we observed that the CFT was significantly lower in all patients. There were also shown the foveal contour restoration and the increment of the superficial FAZ area, and these were significantly greater than those in the preoperative group (0.08±0.04 mm2vs0.12±0.06 mm2,P=0.002;Table 1). The area of the superficial FAZ was also negatively correlated with the CFT in all groups (Figure 2). It can be hypothesized, therefore, that the FAZ is more vulnerable to traction and shear stress by ERM, and restores more slowly after surgery.
This study had some limitations. First, this study had a retrospective design and only used data from a single hospital.Thus, a selection bias may have been introduced. Second,the sample size was small, and the postoperative observation period was relatively short. Therefore, further studies with a larger number of subjects and a longer observation period are needed to confirm these results. Third, although a previous study considered both the SCL and DCL in healthy eyes[10],we analyzed only the SCL in order to measure the FAZ area,because a poor image of the DCL is not suitable for evaluating the FAZ area in preoperative ERM patients. Technological improvements in OCTA technology may allow good visualization of the DCL in ERM patients in future studies.
In conclusion, our study shows that the superficial FAZ was much smaller in ERM eyes than that of the unaffected felloweyes, and the superficial FAZ area increased after ERM surgery. The superficial FAZ area was negatively correlated with the CFT. Contraction or shrinkage of an ERM may cause not only retinal thickening, but also various degrees of distortional force in the inner retinal layer, leading to the reduction and deformation of FAZ area. This distortional and narrow FAZ may not allow the light to be sensed without any dispersion or loss. The results encourage further studies to determine the correlation between the superficial FAZ area and visual function in eyes after ERM surgery.

Figure 2 The relationship between superficial FAZ area and CFT
The area of the preoperative superficial FAZ was strongly negatively correlated with the preoperative CFT (A;P<0.001,rho=-0.763). The areas of the FAZ in the postoperative (B) and control groups (C) were moderately negatively correlated with the respective CFTs (P=0.032,rho=-0.379 andP=0.007,rho=-0.555, respectively).
ACKNOWLEDGEMENTS
Conflicts of Interest:Yoon YS, None; Woo JM, None; Woo JE, None; Min JK, None.
REFERENCES
1 Weale RA. Why does the human retina possess a fovea?Nature1966;212(5059):255-256.
2 Provis JM, Diaz CM, Dreher B. Ontogeny of the primate fovea: a central issue in retinal development.Prog Neurobiol1998;54(5):549-580.
3 Dubis AM, Hansen BR, Cooper RF, Beringer J, Dubra A, Carroll J. Relationship between the foveal avascular zone and foveal pit morphology.Invest Ophthalmol Vis Sci2012;53(3):1628-1636.
4 McDonald HR, Verre WP, Aaberg TM. Surgical management of idiopathic epiretinal membranes.Ophthalmology1986;93(7):978-983.
5 Hillenkamp J, Saikia P, Gora F, Sachs HG, Lohmann CP, Roider J,Bäumler W, Gabel VP. Macular function and morphology after peeling of idiopathic epiretinal membrane with and without the assistance of indocyanine green.Br J Ophthalmol2005;89(4):437-443.
6 Falkner-Radler CI, Glittenberg C, Hagen S, Benesch T, Binder S.Spectral-domain optical coherence tomography for monitoring epiretinal membrane surgery.Ophthalmology2010;117(4):798-805.
7 Niwa T, Terasaki H, Kondo M, Piao CH, Suzuki T, Miyake Y. Function and morphology of macula before and after removal of idiopathic epiretinal membrane.Invest Ophthalmol Vis Sci2003;44(4):1652-1656.
8 Schadlu R, Tehrani S, Shah GK, Prasad AG. Long-term follow-up results of ilm peeling during vitrectomy surgery for premacular fibrosis.Retina2008;28(6):853-857.
9 Mammo Z, Balaratnasingam C, Yu P, Xu J, Heisler M, Mackenzie P, Merkur A, Kirker A, Albiani D, Freund KB, Sarunic MV, Yu DY.Quantitative noninvasive angiography of the fovea centralis using speckle variance optical coherence tomography.Invest Ophthalmol Vis Sci2015;56(9):5074-5086.
10 Samara WA, Say EA, Khoo CT, Higgins TP, Magrath G, Ferenczy S, Shields CL. Correlation of foveal avascular zone size with foveal morphology in normal eyes using optical coherence tomography angiography.Retina2015;35(11):2188-2195.
11 Laatikainen L, Larinkari J. Capillary-free area of the fovea with advancing age.Invest Ophthalmol Vis Sci1977;16(12):1154-1157.
12 Vinekar A, Avadhani K, Sivakumar M, Mahendradas P, Kurian M,Braganza S, Shetty R, Shetty BK. Understanding clinically undetected macular changes in early retinopathy of prematurity on spectral domain optical coherence tomography.Invest Ophthalmol Vis Sci2011;52(8):5183-5188.
13 Seo JH, Yu YS, Kim JH, Choung HK, Heo JW, Kim SJ. Correlation of visual acuity with foveal hypoplasia grading by optical coherence tomography in albinism.Ophthalmology2007;114(8):1547-1551.
14 McAllister JT, Dubis AM, Tait DM, Ostler S, Rha J, Stepien KE,Summers CG, Carroll J. Arrested development: high-resolution imaging of foveal morphology in albinism.Vision Res2010;50(8):810-817.
15 Al-Sheikh M, Akil H, Pfau M, Sadda SR. Swept-source OCT angiography imaging of the foveal avascular zone and macular capillary network density in diabetic retinopathy.Invest Ophthalmol Vis Sci2016;57(8):3907-3913.
16 Balaratnasingam C, Inoue M, Ahn S, McCann J, Dhrami-Gavazi E,Yannuzzi LA, Freund KB. Visual acuity is correlated with the area of the foveal avascular zone in diabetic retinopathy and retinal vein occlusion.Ophthalmology2016;123(11):2352-2367.
17 Coscas F, Glacet-Bernard A, Miere A, Caillaux V, Uzzan J, Lupidi M,Coscas G, Souied EH. Optical coherence tomography angiography in retinal vein occlusion: evaluation of superficial and deep capillary plexa.Am J Ophthalmol2016;161:160-171.
18 Michalewski J, Michalewska Z, Cisiecki S, Nawrocki J. Morphologically functional correlations of macular pathology connected with epiretinalmembrane formation in spectral optical coherence tomography (SOCT).Graefes Arch Clin Exp Ophthalmol2007;245(11):1623-1631.
19 Kim J, Rhee KM, Woo SJ, Yu YS, Chung H, Park KH. Long-term temporal changes of macular thickness and visual outcome after vitrectomy for idiopathic epiretinal membrane.Am J Ophthalmol2010;150(5):701-709.
20 Bovey EH, Uffer S, Achache F. Surgery for epimacular membrane:impact of retinal internal limiting membrane removal on functional outcome.Retina2004;24(5):728-735.
21 Hartmann KI, Schuster AK, Bartsch DU, Kim JS, Chhablani J,Freeman WR. Restoration of retinal layers after epiretinal membrane peeling.Retina2014;34(4):647-654.
22 Pilli S, Lim P, Zawadzki RJ, Choi SS, Werner JS, Park SS. Fourierdomain optical coherence tomography of eyes with idiopathic epiretinal membrane: correlation between macular morphology and visual function.Eye(Lond)2011;25(6):775-783.
23 Suh MH, Seo JM, Park KH, Yu HG. Associations between macular findings by optical coherence tomography and visual outcomes after epiretinal membrane removal.Am J Ophthalmol2009;147(3):473-480.
24 Oster SF, Mojana F, Brar M, Yuson RMS, Cheng L, Freeman WR.Disruption of the photoreceptor inner segment/outer segment layer on spectral domain-optical coherence tomography is a predictor of poor visual acuity in patients with epiretinal membranes.Retina2010;30(5):713-718.
25 Mitamura Y, Hirano K, Baba T, Yamamoto S. Correlation of visual recovery with presence of photoreceptor inner/outer segment junction in optical coherence images after epiretinal membrane surgery.Br J Ophthalmol2009;93(2):171-175.
26 Ooto S, Hangai M, Takayama K, Sakamoto A, Tsujikawa A, Oshima S, Inoue T, Yoshimura N. High-resolution imaging of the photoreceptor layer in epiretinal membrane using adaptive optics scanning laser ophthalmoscopy.Ophthalmology2011;118(5):873-881.
27 Watanabe A, Arimoto S, Nishi O. Correlation between metamorphopsia and epiretinal membrane optical coherence tomography findings.Ophthalmology2009;116(9):1788-1793.
Citation:Yoon YS, Woo JM, Woo JE, Min JK. Superficial foveal avascular zone area changes before and after idiopathic epiretinal membrane surgery.Int J Ophthalmol2018;11(10):1711-1715
DOl:10.18240/ijo.2018.10.21
Accepted:2018-02-23
Received:2017-11-21
Correspondence to:Jung Kee Min. Department of Ophthalmology,Ulsan University Hospital, College of Medicine, University of Ulsan, 290-3 Jeonha-dong, Dong-gu, Ulsan 44033, Republic of Korea. minjungkee75@gmail.com