Posterior chamber phakic intraocular lens for the correction of high myopic anisometropic amblyopia in adults
Jing Zhang1, Jing Zhuang2, Ke-Ming Yu2
1Shenzhen Eye Hospital, Shenzhen Key Laboratory of Ophthalmology, Affiliated Shenzhen Eye Hospital of Jinan University, Shenzhen 518040, Guangdong Province, China.
2State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou 510060, Guangdong Province, China
Abstract
● This study aims to evaluate the clinical results of posterior chamber implantable collamer lens (lCL) implantation in adults with high myopic anisometropic amblyopia.Thirteen patients aged 27.04±7.24y (range 19.2 to 42.5) were studied.lCL implantation was performed in 13 amblyopic eyes.The mean myopic anisometropia was significantly dropped from -10.70±3.02 D preoperatively to +0.09±1.67 D at 1mo postoperatively.The logMAR CDVA at 3d, 1, 3 and mean 9mo postoperatively improved by a mean of 1.69, 2.50, 3.01 and 3.00 lines and gained more than 2 lines accounted for 23.08% (3 eyes), 41.67% (5 eyes), 63.63% (7 eyes) and 55.56% (5 eyes), respectively.The contrast sensitivity of amblyopic eyes was signifcantly increased after surgery.Four patients partially recovered near stereopsis (400” to 100”).There was no severe complications were observed.lCL implantation alone can improve vision, contrast sensitivity, and partial restoration of binocular vision in adult patients with high myopic anisometropia.
● KEYWORDS:phakic intraocular lens; myopic anisometropic;amblyopia; refractive surgery
INTRODUCTION
Amblyopia is a neurodevelopmental ocular disease manifested as monocular and binocular impairments,including reduction of vision, contrast sensitivity, or even loss of stereoscopic vision.It is mainly caused by anisometropia, strabismus, or both.Spectacles or contact lenses are the traditional treatments of eliminating refractive errors for anisometropic amblyopia.Cornea refractive surgeries including photorefractive keratectomy, laserin situkeratomileusis (LASIK), laser-assisted subepithelial keratectomy, femtosecond laser-assistedin situkeratomileusis(FS-LASIK) or small-incision lenticule extraction have been reported as efficacious and safe alternatives to correct high myopic anisometropic amblyopia in children who have failed with spectacles or contact lenses to correct refractive errors[1-3].High myopia over -12 diopters (D) or a thin cornea (residual stromal bed thickness <280 μm) was supposed as contraindications for corneal refractive surgeries.Due to the advantages of reversible, less traumatic, a rapid recovery, and avoiding corneal-related complications, posterior chamber phakic implantable collamer lens (ICL) implantation has become the preferred refractive surgical approach for the patients who were not suitable for corneal refractive surgeries[4-5].Several previous studies[6]also suggested that ICL may be a better surgical option for correcting high myopia in adult patients because of optical advantages, fewer ocular higher order aberrations, better contrast sensitivity compared with LASIK.Previous studies also showed that ICL implantation can be a promising alternative therapy for high myopic anisometropic amblyopia in pediatric patients who have failed with conventional treatments and were not suitable for corneal refraction surgeries[7-8].
Nowadays, amblyopia treatments are not merely restricted to childhood, which is regarded as the critical visual developmental period.A few studies in the literature reported the effectiveness of refractive correction alone by corneal refractive surgeries[9-11], or angle-supported phakic intraocular lens(PIOL)[12-13]and ICL[14]in adult patients with anisometropic amblyopia.Therefore, this study was proposed to further observe the ICL implantation for adults with high myopic anisometropia amblyopia.
SUBJECTS AND METHODS
Thirteen patients (8 men and 5 women) diagnosed with high myopic amblyopia at Zhongshan Ophthalmic Center of Sun Yat-sen University between December 2013 and February 2015 were evaluated.Inclusion criteria were as follows: age at least 18y; between two eyes with refractive errors difference atleast 5.00 D; corrected distance visual acuity (CDVA) below 20/25 (Snellen) in the eye with high refractive errors or the difference of binocular CDVA was no less than two lines;fulfill the indications for ICL implantation.Table 1 shows the preoperative patient demographics.The mean age of the 13 patients at the time of ICL implantation was 27.04±7.24y(range: 19.2 to 42.5).All the study procedures were conducted in accordance with the tenets of the World Medical Association’s Declaration of Helsinki.Ethical approval was obtained from the Ethics Committee of Zhongshan Ophthalmic Center (ethical approval number: 2014MEKY001).
Table 1 Preoperative demographics of adult patients with high myopic amblyopia
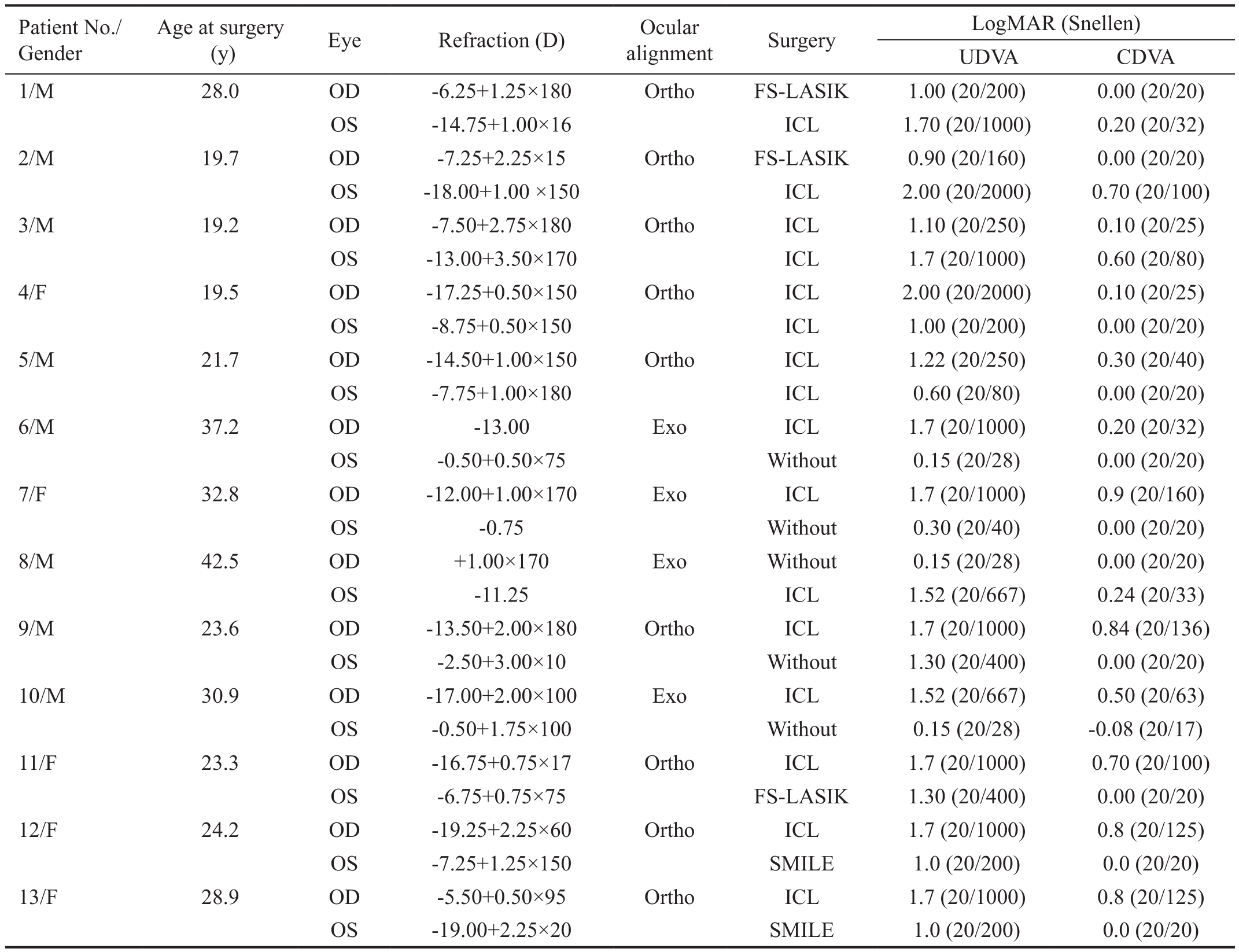
D: Diopters; UDVA: Uncorrected distance visual acuity; CDVA: Corrected distance visual acuity; Ortho: Orthophoria; Exo: Exotropia; Without:Without surgery; ICL: Implantable collamer lens; FS-LASIK: Femtosecond laser-assistedin situkeratomileusis; SMILE: Small-incision lenticule extraction.
Patient No./Gender Age at surgery(y) Eye Refraction (D) Ocular alignment Surgery LogMAR (Snellen)UDVA CDVA 1/M 28.0 OD -6.25+1.25×180 Ortho FS-LASIK 1.00 (20/200) 0.00 (20/20)OS -14.75+1.00×16 ICL 1.70 (20/1000) 0.20 (20/32)2/M 19.7 OD -7.25+2.25×15 Ortho FS-LASIK 0.90 (20/160) 0.00 (20/20)OS -18.00+1.00 ×150 ICL 2.00 (20/2000) 0.70 (20/100)3/M 19.2 OD -7.50+2.75×180 Ortho ICL 1.10 (20/250) 0.10 (20/25)OS -13.00+3.50×170 ICL 1.7 (20/1000) 0.60 (20/80)4/F 19.5 OD -17.25+0.50×150 Ortho ICL 2.00 (20/2000) 0.10 (20/25)OS -8.75+0.50×150 ICL 1.00 (20/200) 0.00 (20/20)5/M 21.7 OD -14.50+1.00×150 Ortho ICL 1.22 (20/250) 0.30 (20/40)OS -7.75+1.00×180 ICL 0.60 (20/80) 0.00 (20/20)6/M 37.2 OD -13.00 Exo ICL 1.7 (20/1000) 0.20 (20/32)OS -0.50+0.50×75 Without 0.15 (20/28) 0.00 (20/20)7/F 32.8 OD -12.00+1.00×170 Exo ICL 1.7 (20/1000) 0.9 (20/160)OS -0.75 Without 0.30 (20/40) 0.00 (20/20)8/M 42.5 OD +1.00×170 Exo Without 0.15 (20/28) 0.00 (20/20)OS -11.25 ICL 1.52 (20/667) 0.24 (20/33)9/M 23.6 OD -13.50+2.00×180 Ortho ICL 1.7 (20/1000) 0.84 (20/136)OS -2.50+3.00×10 Without 1.30 (20/400) 0.00 (20/20)10/M 30.9 OD -17.00+2.00×100 Exo ICL 1.52 (20/667) 0.50 (20/63)OS -0.50+1.75×100 Without 0.15 (20/28) -0.08 (20/17)11/F 23.3 OD -16.75+0.75×17 Ortho ICL 1.7 (20/1000) 0.70 (20/100)OS -6.75+0.75×75 FS-LASIK 1.30 (20/400) 0.00 (20/20)12/F 24.2 OD -19.25+2.25×60 Ortho ICL 1.7 (20/1000) 0.8 (20/125)OS -7.25+1.25×150 SMILE 1.0 (20/200) 0.0 (20/20)13/F 28.9 OD -5.50+0.50×95 Ortho ICL 1.7 (20/1000) 0.8 (20/125)OS -19.00+2.25×20 SMILE 1.0 (20/200) 0.0 (20/20)
Preoperative ocular examinations included slit lamp and fundus,alternate cover test, cycloplegic refraction, noncontact tonometry, OrbscanIIz, and corneal endothelial cell photography; these were conducted on all patients.The size of ICL was determined with a STAAR sizing calculation formula that based on the measurement of anterior chamber depth and horizontal corneal diameter (white to white distance)by Orbscan II Topographer.Early Treatment of Diabetic Retinopathy Study was converted to logMAR notation for uncorrected distance visual acuity (UDVA) and CDVA test.Furthermore, contrast sensitivity and the near stereopsis(Randot Preschool Stereoacuity Test) were also evaluated preoperatively.Contrast sensitivity of both amblyopic eyes and fellow eyes was assessed at 0.5, 2 and 8 cycles per degree(cpd), using previously described Psykinematix psychophysics software (KyberVision, Quebec, Canada) converging on 79.4%accuracy[15-16].
Thirteen high myopic amblyopic eyes and three fellow eyes were treated with ICL surgery (ICL; model V4, Staar Surgical Inc., USA) by the same experienced surgeon (Yu KM).Postoperatively, tobramycin 0.3% dexamethasone 0.1%eyedrops (Tobradex) were administered 4 times a day for 1wk and then 2 times a day for 1wk.Slit-lamp examination,intraocular pressure (IOP), refraction, UDVA, CDVA, contrast sensitivity and near stereopsis, objective vaulting were evaluated at each follow up time except 1d and 1wk.Where possible, endothelial cell counts, fundus evaluations andother examinations were performed.The objective vaulting was assessed using a WaveLight Oculyzer anterior segment analysis system (Alcon, Fort Worth, Texas, USA).
Table 2 Refraction changes over time in adult patients with high anisometropic amblyopia after refractive surgeries
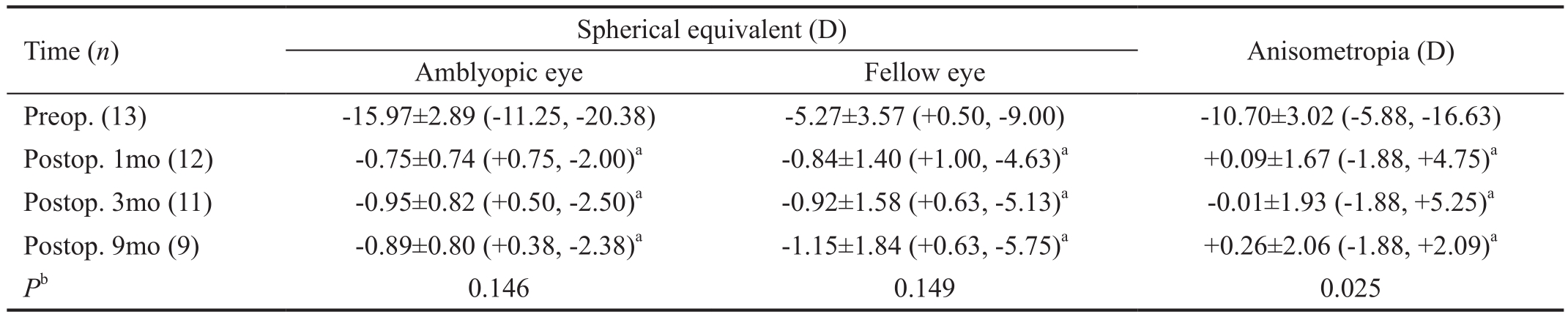
Preop.: Preoperative; Postop.: Postoperative; D: Diopters.aP<0.05 compared with preop.;bPrepresent difference among postop.follow up time.
Time (n) Spherical equivalent (D) Anisometropia (D)Amblyopic eye Fellow eye Preop.(13) -15.97±2.89 (-11.25, -20.38) -5.27±3.57 (+0.50, -9.00) -10.70±3.02 (-5.88, -16.63)Postop.1mo (12) -0.75±0.74 (+0.75, -2.00)a-0.84±1.40 (+1.00, -4.63)a+0.09±1.67 (-1.88, +4.75)aPostop.3mo (11) -0.95±0.82 (+0.50, -2.50)a-0.92±1.58 (+0.63, -5.13)a-0.01±1.93 (-1.88, +5.25)aPostop.9mo (9) -0.89±0.80 (+0.38, -2.38)a-1.15±1.84 (+0.63, -5.75)a+0.26±2.06 (-1.88, +2.09)aPb0.146 0.149 0.025
RESULTS
Patients completed postoperative follow ups in this study at 3d,1, 3mo and the last follow up time [mean: 9.33±2.87 (range 6 to 14)mo] accounted for 100% (13/13), 92% (12/13), 85%(11/13), and 69% (9/13), respectively.
RefractionThe achieved spherical equivalent (SE) at 1mo postoperatively was within ±0.50 D and ±1.00 D of the attempted power, accounting for 69% (9 eyes) and 100%(13 eyes) of patients respectively.Table 2 shows the mean SE of amblyopic eyes, the mean SE of fellow eyes, and that the SE anisometropia were significantly reduced at 1, 3 and approximately 9mo postoperatively (allP<0.05).The SE refraction of both in amblyopic eyes and fellow eyes was not signifcantly changed during about 9mo after surgery (allP>0.05 respectively).However, the SE anisometropia changes was statistically significantly different during about 9mo postoperative follow up (F=4.881,P=0.025).
Visual AcuityThere was a significant improvement for both UDVA and CDVA of the amblyopic eye at 3d, 1, 3 and about 9mo after surgery compared with preoperative (P<0.05 for all) shown in Figure 1A.Both UDVA and CDVA of the amblyopic eye after ICL implantation were significantly increased during about 9mo follow up postoperatively (P<0.05 for all).Figure 1B shows the logMAR CDVA was improved mean 1.69±1.55 (0-5) lines, 2.50±1.51 (0-5) lines, 3.01±1.22(1-5) lines, 3.00±1.50 (1-6) lines at 3d, 1, 3 and about 9mo postoperatively, and gained more than 2 lines accounted for 23.08% (3 eyes), 41.67% (5 eyes), 63.63% (7 eyes) and 55.56% (5 eyes), respectively.No amblyopic eyes lost visual acuity after surgery.
Contrast SensitivityTable 3 shows the changes in contrast sensitivity over time for both eyes in patients after refractive surgeries for anisometropia correction.The contrast sensitivity of 0.5, 2, 8 cpd at 3d and 3mo, 2 cpd and 8 cpd at 1mo and 2 cpd at about 9mo in amblyopic eyes was significantly increased after surgery (allP<0.05).The contrast sensitivity of 8 cpd at 3mo and 0.5 cpd at about 9mo in dominated eyes was signifcantly improved postoperatively (allP<0.05).The contrast sensitivity of 8 cpd in amblyopic eyes and 0.5 cpd in fellow eyes was significantly increased with the followup time (allP<0.05), but other spatial frequencies were not signifcantly changed (P>0.05 for all ).
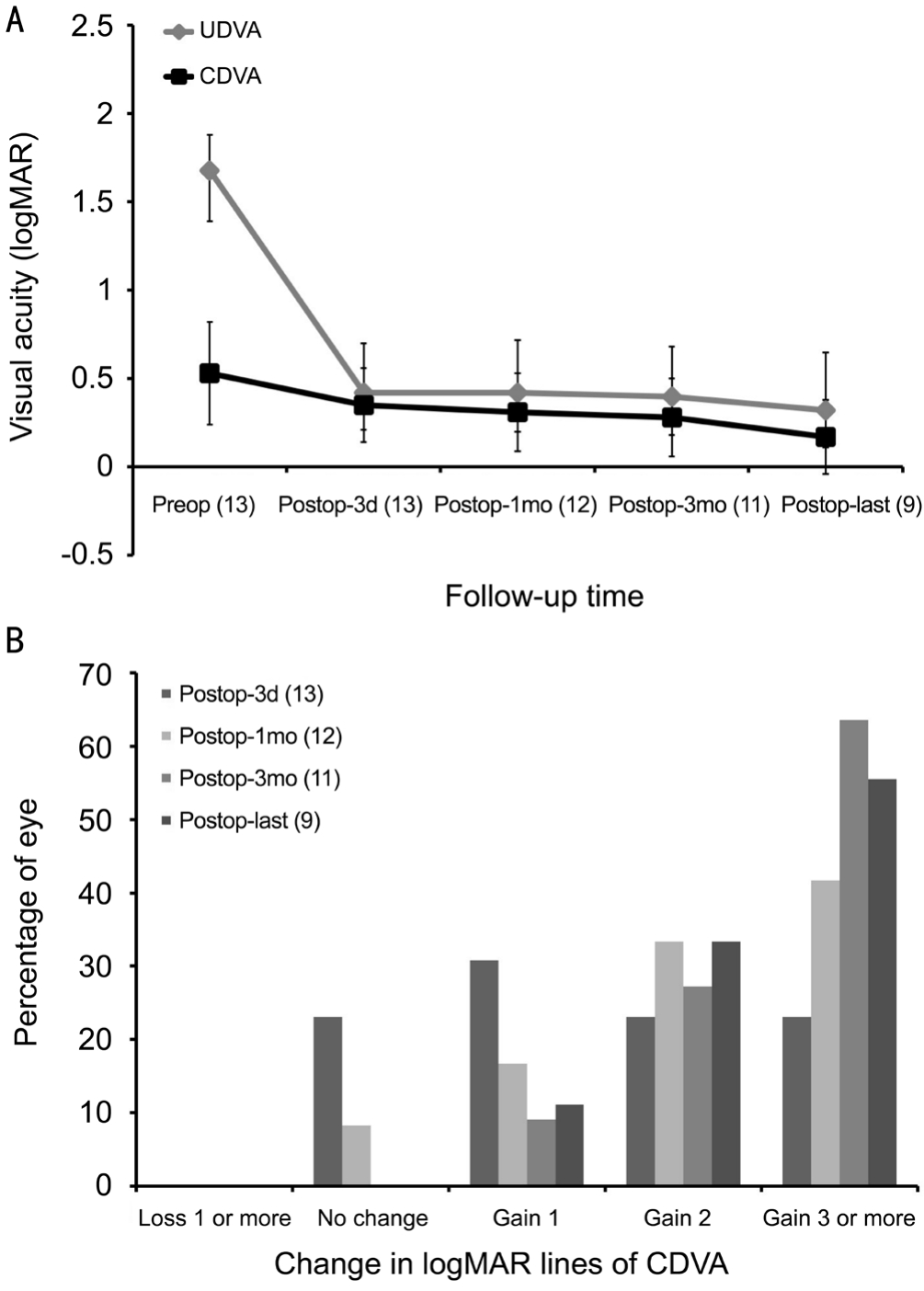
Figure 1 Visual acuity changes in the operated eyes A: Changes of logMAR UDVA and CDVA over time in amblyopic eyes after ICL implantation; B: Changes in lines of logMAR CDVA in amblyopic eyes postoperatively.
StereopsisOnly one patient with 400” near stereopsis preoperatively, and 4 patients (30.8%) recovered to 400” to 100” at approximately 9mo follow up postoperatively.
Intraocular PressureThe IOP for the amblyopic eye was significantly changed from 15.60±3.79 (8, 21) mm Hg preoperatively to 16.38±5.20 (7, 24) mm Hg at 3d, 13.75±4.43(9, 22) mm Hg at 1mo, 12.73±3.52 (5, 17) mm Hg at 3mo,15.38±3.38 (9, 22) mm Hg at about 9mo after surgery,respectively (F=3.069,P=0.032).
Table 3 Changes in contrast sensitivity over time in patients with high anisometropic amblyopia after refractive surgeries
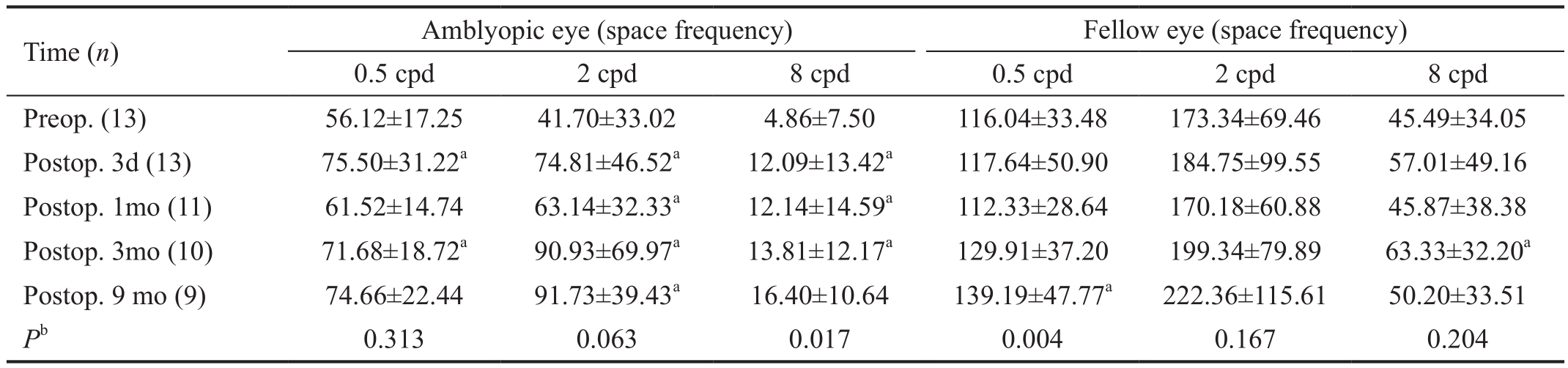
Preop.: Preoperative; Postop.: Postoperative; cpd: Cycle per degree.aP<0.05 compared with preop.significantly difference;bPrepresent difference among postop.follow up time.
Time (n) Amblyopic eye (space frequency) Fellow eye (space frequency)0.5 cpd 2 cpd 8 cpd 0.5 cpd 2 cpd 8 cpd Preop.(13) 56.12±17.25 41.70±33.02 4.86±7.50 116.04±33.48 173.34±69.46 45.49±34.05 Postop.3d (13) 75.50±31.22a74.81±46.52a12.09±13.42a117.64±50.90 184.75±99.55 57.01±49.16 Postop.1mo (11) 61.52±14.74 63.14±32.33a12.14±14.59a112.33±28.64 170.18±60.88 45.87±38.38 Postop.3mo (10) 71.68±18.72a90.93±69.97a13.81±12.17a129.91±37.20 199.34±79.89 63.33±32.20aPostop.9 mo (9) 74.66±22.44 91.73±39.43a16.40±10.64 139.19±47.77a222.36±115.61 50.20±33.51Pb0.313 0.063 0.017 0.004 0.167 0.204
VaultingThe mean vaulting was signifcantly changed from 0.52±0.17 (range, 0.20 to 0.77) mm at 3d, to 0.48±0.16 (range,0.23 to 0.71) mm at 1mo , 0.46±0.16 (range, 0.20 to 0.68) mm at 3mo and 0.40±0.12 (range, 0.23 to 0.60) mm at about 9mo after surgery (F=3.935,P=0.030).
Endothelial Cell CountThe mean endothelial cell count as not significantly changed from 2760.17±276.80(range, 2189.80 to 3217.00) cells/mm2preoperatively to 2799.95±328.83 (range, 2177.80 to 3209.20) cells/mm2at approximately 9mo postoperatively (t=0.661,P=0.525).
ComplicationsTwo patients had transient IOP elevation, and no other intraoperative or postoperative complications were observed.
DISCUSSION
Refractive correction with spectacles, contact lenses or corneal surgeries were reported as effective in adult patients with anisometropic amblyopia[9,17].Agcaet al[9]reported that 14 eyes in 33 adults with myopic anisometropic amblyopia improved two lines or more of CDVA at 6mo after LASIK.Oruçoğlu-Orucovet al[10]also stated that 5 out of 30 myopic eyes in adult with mild to moderate amblyopia gained 2 to 4 lines of CDVA after laser refractive surgery.Unilateral lens extraction was also reported can improve vision for high anisometropic myopia in children and adolescents, however,the incidence of retinal detachments was 3 fold higher than phakic IOL implantation[18].We previous observed 11 children with unilateral high myopic amblyopia[7].The logMAR CDVA of the amblyopic eye was improved by a mean of 2.64 lines at about 8mo after ICL surgery.Alióet al[12]implanted anglesupported PIOL in 59 eyes of 48 patients with anisometropic amblyopia, and 91.5% eyes gained one or more lines of visual acuity.Kwonet al[13]reported the CDVA of 12 eyes with high myopic amblyopia improved an average of 3.92±1.24 lines after angle-supported PIOL implantation.Shiet al[14]also reported the CDVA improved mean 2 lines after ICL implanted for myopic anisometropic amblyopia in 11 adults.In our study,the SE of 13 amblyopic eyes was as high as -15.97±2.89 D that were not suitable for corneal refractive surgeries.The logMAR CDVA increased by a mean of 3.00 lines at 3 and 9mo postoperatively, without anyone lost visual acuity.The contrast sensitivity was also signifcantly increased after ICL implantation.The decimal CDVA of four cases (30.77%)recovered to over 0.8 reaching the cure standard of amblyopia,and the near stereopsis for these patients also recovered to 100” to 400”.Our results agree with the literatures that simple refractive errors correction can improve the visual acuity and contrast sensitivity and partially recover near stereopsis of adult patients with high anisometropia amblyopia.We speculated the reasons for the good optical treatment results after ICL implantation might as follow: firstly, the CDVA of the cured amblyopic eyes in our study was not so bad before surgery;secondly, ICL implantation is superior for the treatment of unilateral myopic anisometropia than spectacle correction for it might eliminate the binocular retinal image size differences and be much closer to the physiological conditions.However,whether the adult patients with residual amblyopia after elimination of anisometropia by refractive surgeries can beneft from amblyopia therapy needs further study.
Potential complications including cataract formation, pupillaryblock glaucoma, and dislocation were previously reported in adults after ICL implantation[5].A continuous reduction of central vault in agreement with previous research was observed in our results[19-20].The vaulting was ranged from 0.23 to 0.60 mm at 9mo after surgery, and no adverse events were observed.An excellent vaulting was defined as 0.25 to 0.75 mm.Excessive and insuffcient vaulting were the risk factors of complications such as pupillary-block glaucoma or cataract formation[21].Temporary mild elevated of IOP was observed and soon resolved.Residues of hyaluronic acid material in anterior chamber, a side effect of topical corticosteroids,and measurement errors of non-contact nometer might be the reasons for transient high IOP.Although endothelial cell count was not significantly lost, and severe postoperative complications were not observed.The patients need to be followed regularly to evaluate the vault and endothelial cell count to avoid severe complications.Recently, the newly ICL V4c with a central hole (STAAR Surgical AG) is widely used to replace the V4 to correct moderate to high myopia in adults which can provide similar results to conventional ICL[22-23].It does not require iridotomy or iridectomy and may also reduce the risk of pupillary block and cataract formation.This newly developed hole ICL implantation appears to be a good option for anisometropia with amblyopia in adults.
Our preliminary results show that ICL implantation can improve visual acuity, contrast sensitivity and partially recover near stereopsis in adult amblyopic patients with high myopic anisometropia.However, there were only a small number of patients with short-term follow up evaluated in our study.Longer time and more patients are still needed to observe the security and effectiveness of ICL implantation for adult anisometropic amblyopia.
ACKNOWLEDGEMENTS
Foundations:Supported by Natural Science Foundation of China (No.81670848; No.81470626).
Conflicts of Interest:Zhang J, None; Zhuang J, None; Yu KM, None.
REFERENCES
1 Autrata R, Rehurek J.Laser-assisted subepithelial keratectomy and photorefractive keratectomy versus conventional treatment of myopic anisometropic amblyopia in children.J Cataract Refract Surg2004;30(1):74-84.
2 Ghanem AA, Moad AI, Nematallah EH, El-Adawy IT, Anwar GM.Laser in situ keratomileusis for treated myopic anisometropic amblyopia in children.Saudi J Ophthalmol2010;24(1):3-8.
3 Zhang J, Yu KM.Femtosecond laser corneal refractive surgery for the correction of high myopic anisometropic amblyopia in juveniles.Int J Ophthalmol2017;10(11):1678-1685.
4 Gomez-Bastar A, Jaimes M, Graue-Hernández EO, Ramirez-Luquin T,Ramirez-Miranda A, Navas A.Long-term refractive outcomes of posterior chamber phakic (spheric and toric implantable collamer lens) intraocular lens implantation.Int Ophthalmol2014;34(3):583-590.
5 Moya T, Javaloy J, Montés-Micó R, Beltrán J, Muñoz G, Montalbán R.Implantable collamer lens for myopia: assessment 12 years after implantation.J Refract Surg2015;31(8):548-556.
6 Kamiya K, Igarashi A, Shimizu K, Matsumura K, Komatsu M.Visual performance after posterior chamber phakic intraocular lens implantation and wavefront-guided laser in situ keratomileusis for low to moderate myopia.Am J Ophthalmol2012;153(6):1178-1186.
7 Zhang J, Li JR, Chen ZD, Yu MB, Yu KM.Phakic posterior chamber intraocular lens for unilateral high myopic amblyopia in Chinese pediatric patients.Int J Ophthalmol2016;9(12):1790-1797.
8 Althomali TA.Posterior chamber toric phakic IOL implantation for the management of pediatric anisometropic amblyopia.J Refract Surg2013;29(6):396-400.
9 Agca A, Ozgürhan EB, Baz O, Bozkurt E, Ozkaya A, Yaşa D, Demirok A.Laser in situ keratomileusis in adult patients with anisometropic amblyopia.Int J Ophthalmol2013;6(3):362-369.
10 Oruçoğlu-Orucov F, Frucht-Pery J, Landau D, Strasman E, Solomon A.LASIK correction of vision in adults with unilateral amblyopia.J Refract Surg2011;27(1):18-22.
11 Kishimoto F, Fujii C, Shira Y, Hasebe K, Hamasaki I, Ohtsuki H.Outcome of conventional treatment for adult amblyopia.Jpn J Ophthalmol2014;58(1):26-32.
12 Alió JL, Ortiz D, Abdelrahman A, de Luca A.Optical analysis of visual improvement after correction of anisometropic amblyopia with a phakic intraocular lens in adult patients.Ophthalmology2007;114(4):643-647.
13 Kwon SW, Moon HS, Shyn KH.Visual improvement in high myopic amblyopic adult eyes following phakic anterior chamber intraocular lens implantation.Korean J Ophthalmol2006;20(2):87-92.
14 Shi MH, Jiang HX, He XY, Zhou W, Wang J.Phakic posterior chamber intraocular lens implantation for myopic anisometropic amblyopia in adults.Rec Adv Ophthalmol2014;34(1):68-71.
15 Li J, Spiegel DP, Hess RF, Chen Z, Chan LY, Deng D, Yu M,Thompson B.Dichoptic training improves contrast sensitivity in adults with amblyopia.Vision Res2015;114:161-172.
16 Chen Z, Li J, Thompson B, Deng D, Yuan J, Chan L, Hess RF, Yu M.The effect of Bangerter filters on binocular function in observers with amblyopia.Invest Ophthalmol Vis Sci2014;56(1):139-149.
17 Tayyab A, Kausar A, Masrur A, Naseem K.Management of anisometropic abmlyopia in adults.J Pak MedAssoc2013;63(2):260-262.
18 Ali A, Packwood E, Lueder G, Tychsen L.Unilateral lens extraction for high anisometropic myopia in children and adolescents.J AAPOS2007;11(2):153-158.
19 Schmidinger G, Lackner B, Pieh S, Skorpik C.Long-term changes in posterior chamber phakic intraocular collamer lens vaulting in myopic patients.Ophthalmology2010;117(8):1506-1511.
20 Alfonso JF, Fernández-Vega L, Lisa C, Fernandes P, González-Meijome J, Montés-Micó R.Long-term evaluation of the central vault after phakic Collamer®lens (ICL) implantation using OCT.Graefes Arch Clin Exp Ophthalmol2012;250(12):1807-1812.
21 Kamiya K, Shimizu K, Komatsu M.Factors affecting vaulting after implantable collamer lens implantation.J Refract Surg2009;25(3):259-264.
22 Huseynova T, Ozaki S, Ishizuka T, Mita M, Tomita M.Comparative study of 2 types of implantable collamer lenses, 1 with and 1 without a central artifcial hole.Am J Ophthalmol2014;157(6):1136-1143.
23 Alfonso JF, Lisa C, Fernández-Vega Cueto L, Belda-Salmerón L,Madrid-Costa D, Montés-Micó R.Clinical outcomes after implantation of a posterior chamber collagen copolymer phakic intraocular lens with a central hole for myopic correction.J Cataract Refract Surg2013;39(6):915-921.
Citation:Zhang J, Zhuang J, Yu KM.Posterior chamber phakic intraocular lens for the correction of high myopic anisometropic amblyopia in adults.Int J Ophthalmol2018;11(11):1870-1874
DOl:10.18240/ijo.2018.11.21
Accepted:2018-08-23
Received:2018-04-03
Correspondence to:Ke-Ming Yu.State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Xianlie Road, Guangzhou 510060, Guangdong Province, China.yukeming@mail.sysu.edu.cn