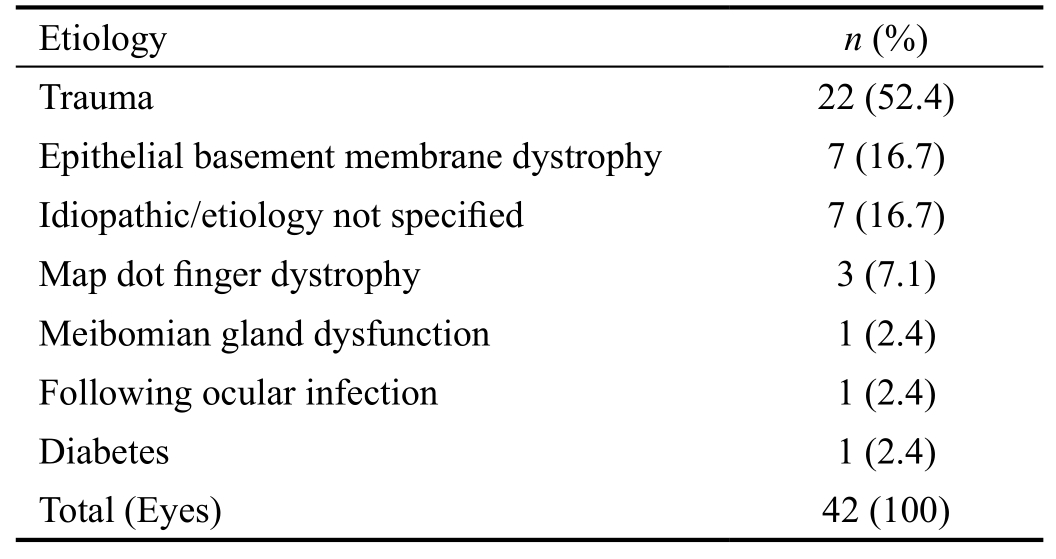
Table 1 Aetiology of recurrent corneal erosion syndrome
·Clinical Research·
Áine Ní Mhéalóid1, Taylor Lukasik2, William Power3, Conor C. Murphy4
1Education and Research Centre, Royal Victoria Eye and Ear Hospital, Dublin D02XK51, Ireland
2School of Medicine, RCSI School of Medicine, Dublin D02VN51, Ireland
3Ophthalmology Department, Royal Victoria Eye and Ear Hospital, Dublin D02XK51, Ireland
4Education and Research Centre, Royal Victoria Eye and Ear Hospital, Dublin D02XK51, Ireland
Recurrent corneal erosion syndrome (RCES) was first described by Hansen in 1872[1]. It is a chronic relapsing clinical disorder involving the corneal epithelium and epithelial basement membrane and is characterized by repeated episodes of breakdown of the corneal epithelium causing moderate to severe eye pain, photophobia, lacrimation, and corneal scarring leading to visual changes. Risk factors include a history of trauma, corneal dystrophies (epithelial basement membrane dystrophy, map-dot-fingerprint dystrophy), meibomian gland dysfunction, previous ocular infection, dry eyes and diabetes.Conservative treatments of RCES include topical lubricants,antibiotic ointments, patching, cycloplegia, bandage contact lenses (BCL) and metalloproteinase inhibitors[2-3]. For patients who are refractory to medical treatment, interventional treatment such as manual epithelial debridement, diamond burr super ficial keratectomy, anterior stromal micropuncture,phototherapeutic keratectomy (PTK) and alcohol delamination(ALD) of the corneal epithelium are indicated[3]. Treatments directed at the pathogenesis of RCES such as substance P-derived peptide with insulin like growth factor-1 (ILGF-1)[4]and autologous serum[5]drops have also been studied.
The aims of this study were to evaluate the outcomes of ALD in the treatment of RCES and to implement a standardized treatment protocol for this condition utilizing evidence based practice and the findings of an internal audit.
The ethical principles outlined in the Declaration of Helsinki(2008) were adhered to in carrying out this research. Oral consent was obtained from the participants and they did not receive a stipend. The population for this audit was obtained retrospectively through medical record code searches for patients diagnosed with RCES, who were treated with ALD between January 2006 and March 2016 in the Royal Victoria Eye and Ear Hospital (RVEEH), Dublin, Ireland. In this institution, patients have 20% alcohol applied to the cornea with the use of a well for 40s. The cornea is then washed with sterile balanced salt solution and the epithelium is debrided. A BCL is inserted and patients are discharged on Pred Forte 1%and minims chloramphenicol 0.5% eye drops, along with oral analgesia. They are reviewed one week later in the Outpatient Department. Outcome criteria were established based on standards from other studies in the medical literature. These included, a treatment success rate of at least 72% (defined as complete resolution of symptoms one month after treatment)[2,6-7], a postoperative complication a rate of <5%(mainly infective keratitis[8-9]and subepithelial haze[6]), and the absence of any detrimental effect on visual acuity in ≥95% of patients.
Data was analyzed using Microsoft Excel (Microsoft Excel for Mac Version 15.18 2015, Seattle Washington, USA)and GraphPad Prism (GraphPad Prism version 7 for Mac,GraphPad Software, La Jolla California, USA). Statistical significance was attributed when P<0.05.
A treatment algorithm was established based on available resources in the Irish public hospital system.
A total of 42 eyes of 40 patients were included in this study. The mean age at the time of ALD was 41.17±13.44y,which is consistent with the literature showing middle-aged predominance[10-13]. Patients were followed for an average of 12.8±15.65mo. The majority were female (52.5%, n=21) and the majority of eyes treated with ALD were left eyes (62.9%,n=26). The aetiology of RCES in our population is outlined in Table 1, with trauma comprising the largest subgroup (n=22).There were no intraoperative or postoperative complications.Conservative treatment was initiated in all patients before ALD was proposed, with lubricants and bandage contact lenses being the most frequent choices.
Treatment was successful in 73.8% (n=31) of eyes and 75.0%(n=30) of patients. Recurrence occurred in 26.2% of eyes at an average of 10.41±12.63mo. The aetiology of recurrent cases is summarised in Table 2.
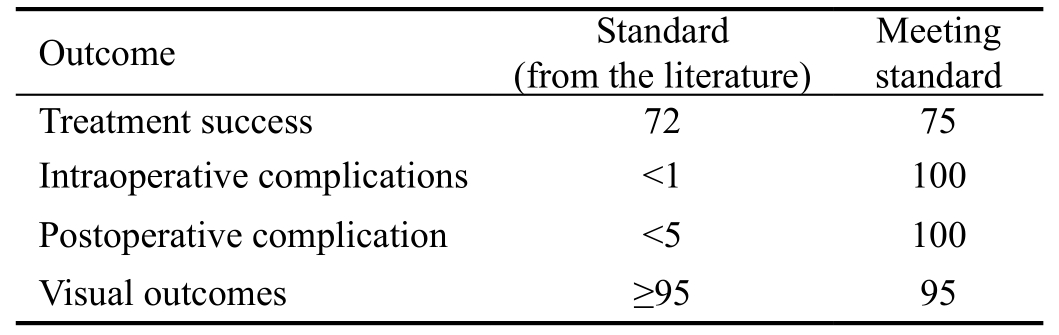
Postoperatively, 95% (n=38) of patients retained or improved their best corrected visual acuity (BCVA) at their last followup. Preoperatively, the mean logMAR BCVA was 0.20±0.08,which improved postoperatively to a mean logMAR BCVA of 0.058±0.058 (P<0.0001) at the latest documented follow-up.The two patients who did not meet this standard both lost one line of vision. Table 3 displays a summary of outcomes.
In 2001, Shah et al[14]reported the use of ALD in preparation for photorefractive keratectomy (PRK) and laser assisted sub-epithelial keratectomy (LASEK). In LASEK patients who underwent ALD, the epithelium was more difficult toremove in the event of retreatment. This led to a 12-patient trial published in 2006 by Dua et al[2]. describing ALD as a novel treatment for RCES. Seventy-five percent of patients responded to treatment. A prospective study by Singh et al[6],which included 20 RCES patients, confirmed ALD of the corneal epithelium as a viable treatment option for RCES refractive to conservative treatment.
Table 1 Aetiology of recurrent corneal erosion syndrome
Table 2 Primary aetiology of treatment failures
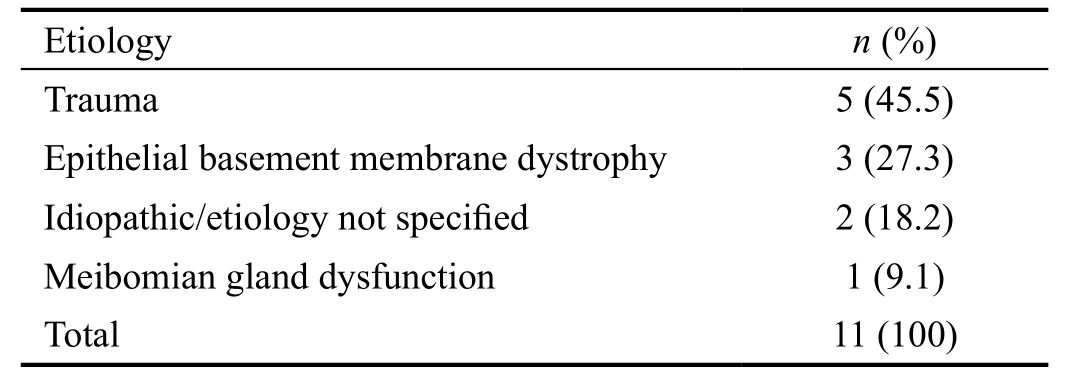
Table 3 Summary of outcomes %
This audit confirms that the majority of patients receiving ALD as a treatment for RCES at the RVEEH meet the safety and efficacy standards as described in the medical literature. The two patients whose vision was negatively impacted upon only lost 1 line of BCVA at 2 and 5mo post-operatively. There was no overt reason for this visual loss as both patients’ corneas recovered adequately after treatment. The loss could have been due to inter-examiner variability or natural fluctuations in patients’ level of vision between clinic appointments. In this audit, trauma and epithelial basement membrane dystrophy(EBMD) were the most common causes of RCES, which is in keeping with the medical literature[3,12,15-16].
We have drafted a number of recommendations to be used locally for such patients. Firstly, the patients’ level of pain should be quantified in the clinical notes, for example, on a Likert scale. This helps in determining successful or partially successful treatment outcomes (those patients who do not have complete resolution of symptoms, but who experience a reduction in symptom frequency and intensity[2,6].
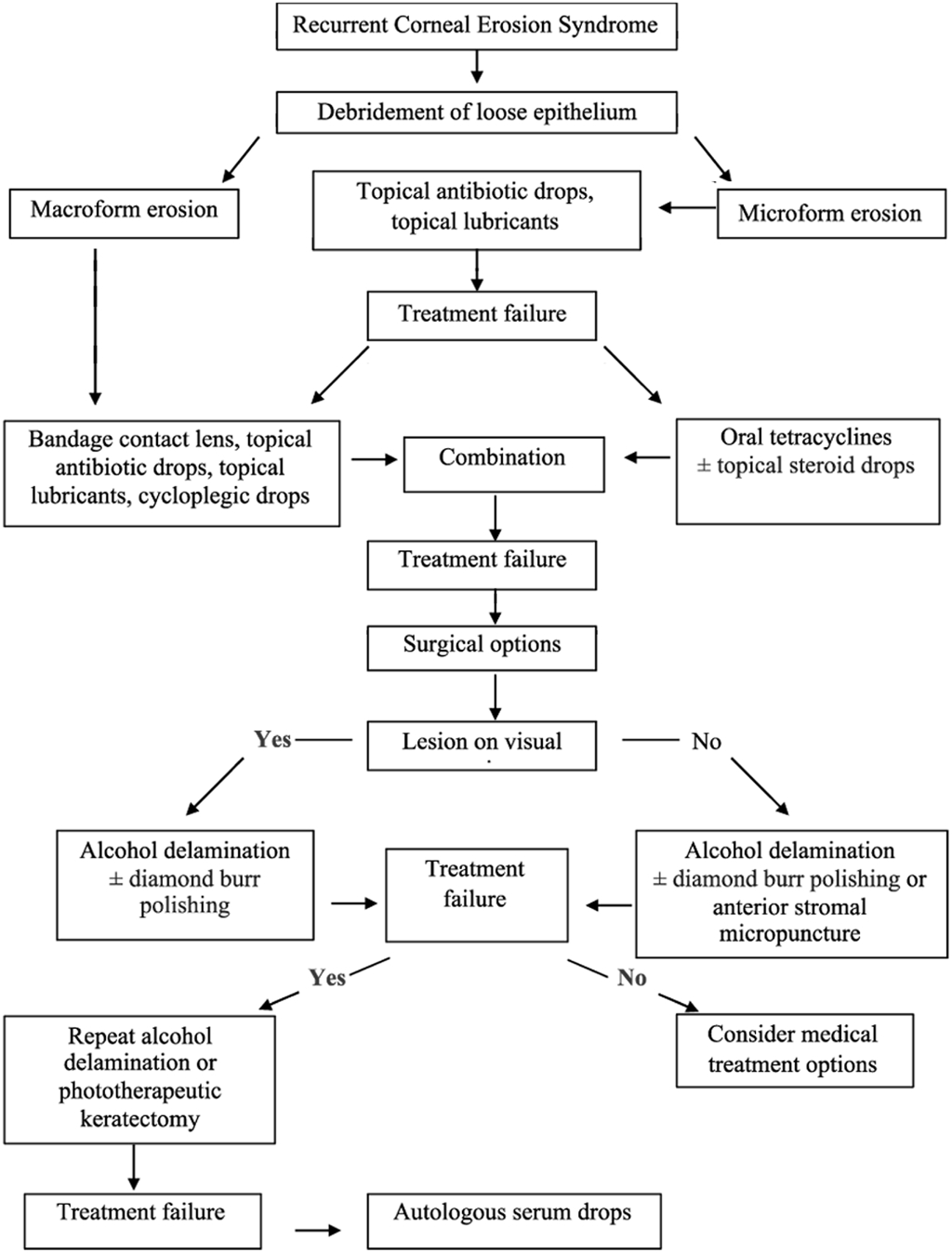
Figure 1 Treatment algorithm for recurrent corneal erosion syndrome.
Oral matrix metalloproteinase (MMP) inhibitors such as oral doxycycline were sparingly used in the care of patients in this audit. MMPs are degradative enzymes found to have an important role in corneal wound healing by clearing damaged matrix during epithelization[17-18]. Garrana et al[19]found that MMP levels, specifically MMP-2 and MMP-9, are elevated in RCES patients compared to those with normal corneal tissue.This excess protease activity can lead to chronic non-healing wounds. In a study of combination treatment consisting of oral doxycycline and topical fluorometholone, 73% of patients were symptom free 6mo after cessation of treatment[20]. There may also be a combined synergistic effect in patents with meibomian gland dysfunction (MGD), where both RCES and MGD are treated with tetracycline antibiotics.
Currently, there is no gold standard for the treatment of RCES.We have composed a treatment protocol for our hospital taking into account the resources available and cost-effectiveness(Figure 1). In conclusion, ALD is a safe, efficacious and cost-effective way of managing RCES that is refractory to medical therapies.
We thank the staff and patients of the Royal Victoria Eye and Ear Hospital, Dublin, Ireland.
Conflicts of Interest: Ní Mhéalóid Á,None;Lukasik T,None;Power W,None;Murphy CC,None.
REFERENCES
1 Hansen E. On den intermitterende keratitis visicularis neuralgica af traumatisk oprindelse.Hospitals Tindende1872;201-203.
2 Dua HS, Lagnado R, Raj D, Singh R, Mantry S, Gray T, Lowe J. Alcohol delamination of the corneal epithelium: an alternative in the management of recurrent corneal erosions.Ophthalmology2006;113(3):404-411.
3 Ramamurthi S, Rahman MQ, Dutton GN, Ramaesh K. Pathogenesis,clinical features and management of recurrent corneal erosions.Eye(Lond)2006;20(6):635-644.
4 Benitez-Del-Castillo JM, Rodríguez-Bayo S, Fontan-Rivas E, Martinezde-la-Casa JM, Garcia-Sanchez J. Treatment of recurrent corneal erosion with substance P-derived peptide and insulin-like growth factor I.Arch Ophthalmol2005;123(10):1445-1447.
5 del Castillo JM, de la Casa JM, Sardiña RC, Fernández RM, Feijoo JG,Gómez AC, Rodero MM, Sánchez JG. Treatment of recurrent corneal erosions using autologous serum.Cornea2002;21(8):781-783.
6 Singh RP, Raj D, Pherwani A, Lagnado R, Abedin A, Eatamadi H,Mathew M, Dua HS. Alcohol delamination of the corneal epithelium for recalcitrant recurrent corneal erosion syndrome: a prospective study of efficacy and safety.Br J Ophthalmol2007;91(7):908-911.
7 Chan E, Jhanji V, Constantinou M, Amiel H, Snibson GR, Vajpayee RB.A randomised controlled trial of alcohol delamination and phototherapeutic keratectomy for the treatment of recurrent corneal erosion syndrome.Br J Ophthalmol2014;98(2):166-171.
8 Saini A, Rapuano CJ, Laibson PR, Cohen EJ, Hammersmith KM.Episodes of microbial keratitis with therapeutic silicone hydrogel bandage soft contact lenses.Eye Contact Lens2013;39(5):324-328.
9 Brown SI, Bloom field S, Pearce DB, Tragakis M. Infections with the therapeutic soft lens.Arch Ophthalmol1974;91(4):275-277.
10 Brown N, Bron A. Recurrent erosion of the cornea.Br J Ophthalmol1976;60(2):84-96.
11 Hope-Ross MW, Chell PB, Kervick GN, McDonnell PJ. Recurrent corneal erosion: clinical features.Eye (Lond)1994;8(Pt 4):373-377.
12 Diez-Feijóo E, Grau AE, Abusleme EI, Durán JA. Clinical presentation and causes of recurrent corneal erosion syndrome: review of 100 patients.Cornea2014;33(6):571-575.
13 Reidy JJ, Paulus MP, Gona S. Recurrent erosions of the cornea:epidemiology and treatment.Cornea2000;19(6):767-771.
14 Shah S, Sebai Sarhan AR, Doyle SJ, Pillai CT, Dua HS. The epithelial flap for photorefractive keratectomy.Br J Ophthalmol2001;85(4):393-396.
15 Watson SL, Lee MH, Barker NH. Interventions for recurrent corneal erosions.Cochrane Database Syst Rev2012;(9):CD001861.
16 Hykin PG, Foss AE, Pavesio C, Dart JK. The natural history and management of recurrent corneal erosion: a prospective randomised trial.Eye (Lond)1994;8(Pt 1):35-40.
17 Sivak JM, Fini ME. MMPs in the eye: emerging roles for matrix metalloproteinases in ocular physiology.Prog Retin Eye Res2002;21(1):1-14.
18 Wong TT, Sethi C, Daniels JT, Limb GA, Murphy G, Khaw PT. Matrix metalloproteinases in disease and repair processes in the anterior segment.Surv Ophthalmol2002;47(3):239-256.
19 Garrana RM, Zieske JD, Assouline M, Gipson IK. Matrix metalloproteinases in epithelia from human recurrent corneal erosion.Invest Ophthalmol Vis Sci1999;40(6):1266-1270.
20 Wang L, Tsang H, Coroneo M. Treatment of recurrent corneal erosion syndrome using the combination of oral doxycycline and topical corticosteroid.Clin Exp Ophthalmol2008;36(1):8-12.
Correspondence to:Áine Ní Mhéalóid. Education and Research Centre, Royal Victoria Eye and Ear Hospital, Adelaide Road,Dublin D02XK51, Ireland. ainenimhealoid@rcsi.ie
Received:2018-03-09 Accepted: 2018-04-16
Abstract ● AlM: To evaluate the outcomes of alcohol delamination(ALD) of the corneal epithelium for the treatment of recurrent corneal erosion syndrome (RCES) and to implement a standardized treatment protocol for this condition utilizing evidence based practice and the findings of an internal audit.● METHODS: A retrospective analysis of 42 eyes of 40 patients diagnosed with RCES who were treated with ALD between January 2006 and March 2016 was conducted.Patients had 20% alcohol applied to the cornea with the use of a well for 40s. Patients were reviewed one week later in the Outpatient Department. Outcome criteria were established based on standards from other studies in the medical literature. These included, a treatment success rate of at least 72% (defined as complete resolution of symptoms one month after treatment), a postoperative complication a rate of <5% (mainly infective keratitis, and subepithelial haze), and the absence of any detrimental effect on visual acuity in ≥95% of patients.● RESULTS: The mean age at the time of ALD was 41.17±13.44y. Patients were followed for an average of 12.8±15.65mo. The majority were female (52.5%, n=21) and the majority of eyes treated with ALD were left eyes (62.9%,n=26). Trauma was the primary aetiology in our study population. Treatment was successful in 73.8% (n=31) of eyes and in 75% (n=30) of patients. Recurrence occurred in 26.2% of eyes at a mean of 10.41±12.63mo post treatment.● CONCLUSlON: ALD is an efficacious and cost-effective primary surgical intervention for RCES.
● KEYWORDS:recurrent corneal erosion; alcohol delamination;corneal abrasion; corneal trauma; corneal dystrophy
DOl:10.18240/ijo.2018.07.09
Citation:Ní Mhéalóid Á, Lukasik T, Power W, Murphy CC. Alcohol delamination of the corneal epithelium for recurrent corneal erosion syndrome. Int J Ophthalmol 2018;11(7):1129-1131