
Figure 1 Normal anterior segment images obtained by 25 MHz and 50 MHz UBM A, B: Normal axial and longitudinal anterior segment images obtained by 25 MHz UBM; C, D: Normal axial and longitudinal anterior segment images obtained by 50 MHz UBM.
Ming-Yu Shi, Xiao Han, Jin-Song Zhang, Qi-Chang Yan
Department of Ophthalmology, the Fourth Affiliated Hospital of China Medical University, Eye Hospital of China Medical University, the Key Laboratory of Lens Research in Liaoning Province, Shenyang 110005, Liaoning Province, China
The lens is an important part of the refractive media in the eye. Its related conditions and diseases, such as cataracts, dislocation, and trauma, seriously affect vision.Until now, the slit lamp is still the major means to observe the lens morphology and diagnose its related diseases[1]. But the slit lamp is an optical inspection device, which is easily affected by the opacity degree of the refractive media and the pupil size. Some anterior segment diseases, such as corneal leukoplakia, hyphema, occlusion of pupil, etc. all can affect the complete observation of lens. In recent years, developments in modalities for anterior segment inspection, such as anterior segment optical coherence tomography (AS-OCT), the Pentacam, and Orbscan II, have allowed clinicians to visualize the anterior segments in cross-section. However, like the slit lamp, these modalities are also optical devices that have some limitations on the overall displaying the lens. So they are often used to measure and compare the anterior segment parameters[2-4], and few studies have evaluated the shape of the lens and its related diseases.
With the emergence of ultrasound biomicroscopy (UBM)[5-6],which has a high frequency transducer, ophthalmologists can obtain information about the lens. However, because the frequency of UBM usually is 50-100 MHz, its penetration is only 3-5 mm[7], so it cannot display a complete clinical lens image. The best method to completely visualize the lens, diagnose diseases, and design a reasonable treatment plan has increasingly become a matter of concern among ophthalmologists. The 25 MHz UBM is a novel ultrasonic diagnostic device that works the same principle as 50 MHz UBM, its frequency is lower, but the depth of penetration is much higher (9-10 mm), and its ultrasonic focus is on the lens.Thus it is possible to acquire high-quality images of the lens.To the best of our knowledge, information regarding these two different frequencies of UBM is scarce. This prospective comparison will discuss these two different imaging modalities and their role in the diagnosis and management of the lens.
Figure 1 Normal anterior segment images obtained by 25 MHz and 50 MHz UBM A, B: Normal axial and longitudinal anterior segment images obtained by 25 MHz UBM; C, D: Normal axial and longitudinal anterior segment images obtained by 50 MHz UBM.
A total of 302 patients (455 eyes) were randomly selected,including 155 females (51.3%) and 147 males (48.7%), from November 2014 to May 2015. Patient age ranged from 5 to 89y(mean±SD: 61.0±17.7y). Among them, 10 patients (20 eyes)were normal, 266 patients (403 eyes) had cataracts, 12 patients(14 eyes) exhibited lens dislocation, 1 patient (2 eyes) had postoperative implantable collamer®lenses (ICL), 7 patients(10 eyes) had glaucoma, 5 patients (5 eyes) had postoperative glaucoma, 1 patient (1 eye) was aphakic, and 1 patient (1 eye)had an intraocular lens (IOL). All subjects underwent 25 MHz(MD-320, MEDA Co., Ltd. Tianjin, China) and 50 MHz panoramic UBM (MD-300L, MEDA Co., Ltd. Tianjin, China)examinations to obtain axial and longitudinal images of the lens,and the anterior segment parameters were measured at the Eye Hospital of China Medical University (Shenyang, Liaoning Province, China). All subjects were fully informed of the details and possible risks of the examination. Written informed consent was obtained from all subjects before the examination following the tenets of the Declaration of Helsinki. The study was approved by the Ethics Committee of the Fourth Affiliated Hospital of China Medical University and registered at www.chictr.org.cn (study registration No. ChiCTR-DOD-15007603).The axial section images of UBM included four directions:12:00-6:00, 3:00-9:00, 4:30-10:30, and 7:30-1:30. The anterior segment parameters included the central corneal thickness(CCT), central anterior chamber depth (ACD), and central lens thickness (CLT). The two UBM scanners were equipped with a 25 MHz and a 50 MHz transducer, allowing 4-5 mm and 9-10 mm tissue penetration, respectively, and an axial resolution of approximately 50 μm. An examination technique similar to conventional gray-scale sonography immersion was employed. The patients were placed in a supine position after super ficial anesthesia. A sterile scleral cup was placed into the conjunctival sac and filled with distilled water as a coupling agent. The interval between these two frequency UBMs examination was 10min. All subjects were in the same indoor light and watching distance during examination, one skilled operator (Shi MY) performed all sonograms and measured the anterior segment parameters. Each anterior segment parameters were measured three times and taken the average value, and all data were obtained with measuring software preassembled in these two UBMs after all images collection and storage, not the real time measurement.
Statistical analysis was performed using SPSS 19.0 for Windows (SPSS, Inc., IBM Armonk, New York, USA), and the results are presented as mean±SD along with the 95%confidence intervals (CI). We used paired t-tests to analyze the differences. A value of P<0.05 was considered statistically significant. B&A plot analysis was used to analyze the agreement of the two UBMs in measuring the anterior segment parameters.
The normal anterior segments on 25 MHz and 50 MHz UBM images are shown in Figure 1. The 25 MHz UBM axial section image revealed that the anterior and posterior capsular lens appeared as two smooth arc lines in strong echo, and no echo was present inside the normal lens, the zonule was visible as a thin and weak stripe-like echo (Figure 1A). On 50 MHz UBM axial section image, the echoes of the lens were weaker than those of 25 MHz UBM, and the zonule was barely visible(Figure 1C). Other anterior segments, such as the cornea, iris,and ciliary body, were displayed more clearly on 50 MHz than on 25 MHz UBM images (Figure 1B, 1D). In the longitudinal section, the image obtained by 25 MHz UBM was fuzzy, and the anterior segments and chamber angle could not be clearly distinguished.
Lens-related disease images obtained by 25 MHz UBM and 50 MHz UBM are shown in Figures 2, 3. Figure 2 display several types of cataracts, including age-related cataract (Figure 2A, 2D), traumatic cataract (Figure 2B, 2E) and subluxated lens with cataract (Figure 2C, 2F). All types of cataracts display different imaging characteristics on 25 MHz UBM, which can display the whole opacity of the lens. Compared to 25 MHz UBM, 50 MHz UBM only shows part of the lens and cannot distinguish the types of cataracts. For traumatic cataracts, the rupture of the posterior capsule and its surrounding lesions are clearly visible via 25 MHz UBM, but the lesions are not shown on 50 MHz UBM. The image features of subluxated lens can be shown clearly in the axial section by 25 MHz UBM, but it cannot be shown intuitively in the same direction of scanning by 50 MHz UBM. Figure 3 shows images of some other lensrelated diseases obtained by 25 MHz UBM, such as IOL,postoperative ICL, and aphakic eye. The relationship between the IOL or ICL and its surrounding tissue is shown clearly by 25 MHz UBM. The mean values of the anterior segment parameters in four axial sections obtained by 25 MHz UBM and 50 MHz UBM were shown in Table 1. No statistically significant differences in the four axial sections were found between groups.
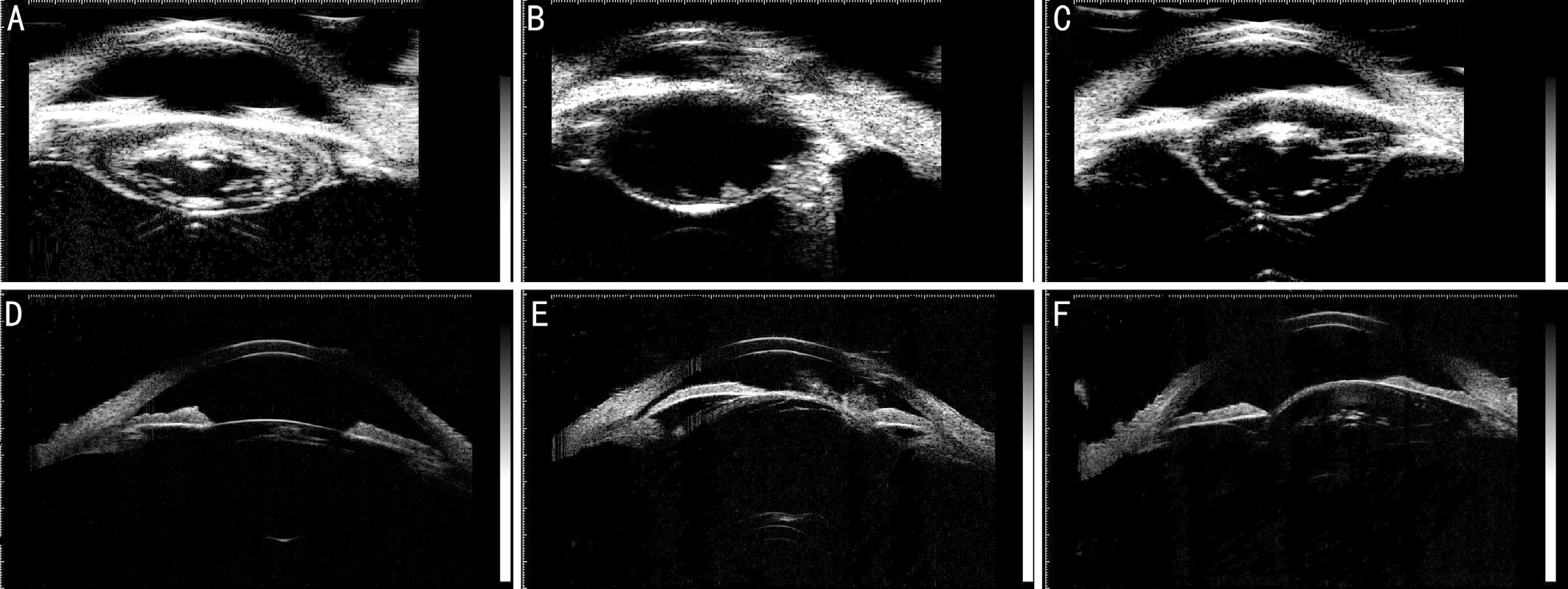
Figure 2 Cataract images obtained by 25 MHz and 50 MHz UBM A-C: Cataract images obtained by 25 MHz UBM; D-F: Cataract images obtained by 50 MHz UBM. From left to right was age-related, traumatic cataract and subluxated lens with cataract, respectively.

Figure 3 Other lens-related diseases images obtained by 25 MHz UBM A: IOL; B: Postoperative ICL; C: Aphakic eye.
Table 1 The means of anterior segment parameters in four axial sections obtained by 25 MHz UBM and 50 MHz UBM
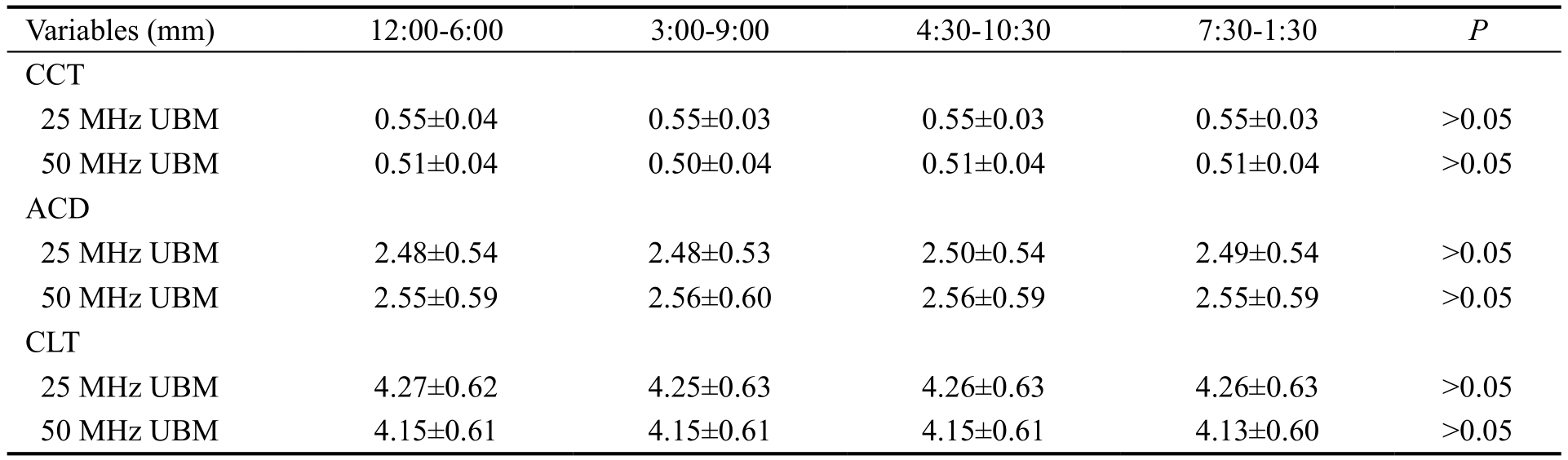
CCT: Central corneal thickness; ACD: Anterior chamber depth; CLT: Central lens thickness.
The means of the anterior segment parameters obtained using 25 and 50 MHz UBM were as follows: CCT: 0.55±0.03 and 0.51±0.04 mm, respectively; ACD: 2.48±0.54 and 2.56±0.56 mm, respectively; and CLT: 4.26±0.62 and 4.15±0.56 mm, respectively. A statistically significant difference was found between the results obtained with 25 MHz UBM and those obtained with 50 MHz UBM (P<0.004). But these two devices had a good agreement in measuring the anterior segment parameters (Figure 4).
UBM is a noninvasive imaging modality that allows for the real-time visualization of anterior segment tissues with microscopic resolution and provides information about the size and nature of the lesion, permitting a presumptive diagnosis[8-12]. In general, the transducer frequency is 50-100 MHz, and the transducer focus is on the surrounding iris; therefore, the anterior segments, such as the cornea, iris,and ciliary body and the anterior capsule of the lens, can be displayed clearly. The characteristics of ultrasonic frequency include a higher frequency and increased resolution, but reduced penetration[13]. As a result, except for the anterior capsule of the lens and a small portion of posterior lens capsule, other parts of the lens can hardly be imaged by 50 MHz UBM. Currently, with the emergence of 25 MHz UBM,which has a relatively low ultrasound frequency and increased penetration, it is possible to observe the overall morphology of the lens. In this prospective study, we verified this presumption by comparing these two UBM frequencies.
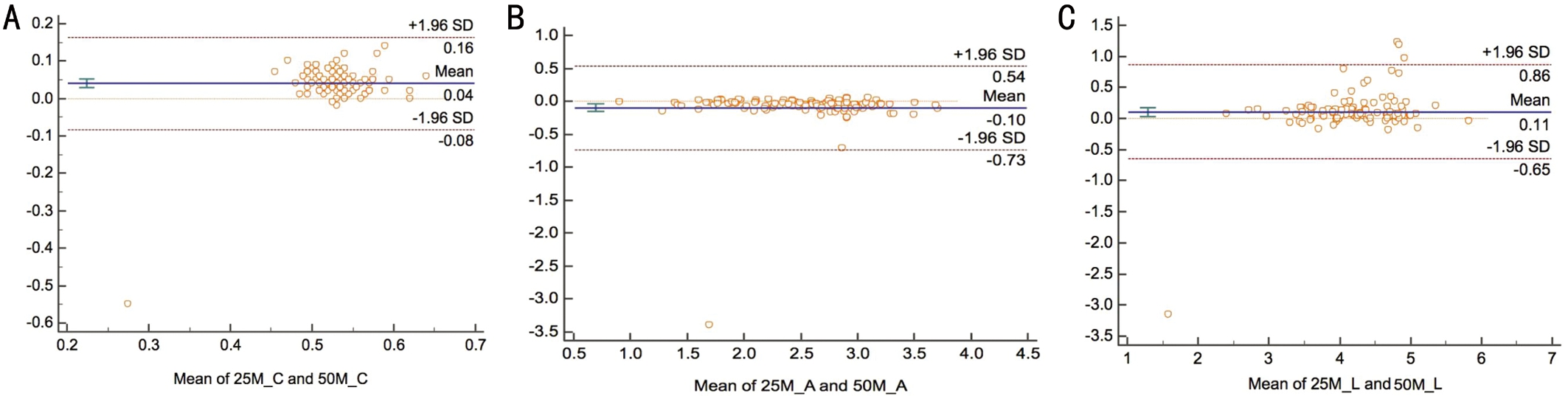
Figure 4 Agreement comparison of anterior segment parameters between 25 MHz UBM and 50 MHz UBM A: CCT; B: ACD; C: CLT.
To completely observe the lens and its lesions, four axial images were captured, and no statistically significant differences were observed between different directions and parameters for 25 MHz and 50 MHz UBM images. Therefore, the mean values of the anterior segment parameters in the four axial sections were used to compare 25 MHz and 50 MHz UBM,and a statistically significant difference was observed between these two frequencies. The tissue images before the anterior surface of the lens were more obscure with the use of 25 MHz UBM due to its lower resolution than on 50 MHz UBM, which may lead to differences in measurements of the CCT and central ACD. However, 25 MHz UBM has a lower frequency with better penetration, and the focus of the transducer is concentrated on the lens. Thus, the complete shape of the lens is displayed more clearly than on 50 MHz UBM. The imaging quality of the posterior lens pole obtained with 50 MHz UBM was greatly affected by the thickness and opacity degree of the lens, especially in most intumescent and nuclear cataract, the posterior lens pole was showed as a dark hypoecho, which may be the reason why the mean CLT of 50 MHz UBM was lower than that obtained by 25 MHz UBM. Our study results showed that there were good agreements between these two different frequencies UBM for anterior segment inspection, which is in accord with the previous researches on comparison of anterior segment parameter among different anterior segment modalities[14-16]. The two UBMs have the same ultrasonic work principle except for different transducer frequency and ultrasound focus, so the anterior segment parameters obtained with these two UBMs are comparable, and they can replace each other to some extent. There is still no gold standard exists for the measurement of anterior segment parameters till now,and it is possible that 50 MHz UBM underestimates the CLT,therefore, the CLT obtained using 25 MHz UBM can replace the lens parameter of 50 MHz UBM and provide a reliable reference for the studies on lens morphology and related diseases.
In the present study, in order to reduce the measurement errors that were led by morphological changes because of long time constriction in eyes with eyecup, every patient had a ten minutes rest between the two UBMs examination. Moreover,all subjects in the same indoor environment and watching distance, one skill operator performed all examinations and measurement, which ensure the consistency of all inspection conditions. However, for other anterior segments in longitudinal sections, 25 MHz UBM does not produce an ideal image and is thus not suitable for imaging corneal diseases,glaucoma, and other anterior segment-related diseases.Therefore, longitudinal section images and parameters were not thoroughly measured in this study.
Due to its advantage of the ability to show the entire lens, 25 MHz UBM is an ideal method to study the lens and its related diseases, especially cataracts. Cataracts represent one of the most well-known disabling eye conditions, and the appearance of a cataract seems to be a result of biochemical changes in the lens[17]. Observation and diagnosis have mainly relied on slit lamp examinations and medical history. Because the anatomical location of the lens is behind the iris, only a portion of the lens can be seen via a slit lamp; even after mydriasis, the lens periphery still cannot be visualized. Using 25 MHz UBM without mydriasis, the entire lens section can be observed visually. In the axial section images obtained by 25 MHz UBM, the opacity of the lens is displayed very clearly, which is crucial for examining cataract formation and clinical classification. Age-related cataracts are the most common type of cataract, and according to the Lens Opacities Classification System (LOCS III) and clinical manifestations, age-related cataracts are classified into three types: cortical, posterior subcapsular, and nuclear cataracts[18-19]. This classification system, which is based on slit lamp standard photographs after dilation, is susceptible to a variety of interpretations by different observers, which might compromise its reproducibility[20]. The use of 25 MHz UBM provides an effective, objective imaging basis for LOCS III, and each type of age-related cataract displays intuitive ultrasonic characteristics on 25 MHz UBM.
In addition to age-related cataracts, other types of cataracts,such as traumatic cataracts, could be objectively imaged using 25 MHz UBM. Determining preoperatively the presence of an intact posterior lens capsule through echographic confirmation assists the physician in surgical planning[21]. In the present study, 6 eyes with traumatic cataracts were found the tear of posterior lens capsule using 25 MHz UBM and they were confirmed intraoperative, compared with 25 MHz UBM,50 MHz UBM cannot display the full posterior lens capsule except a small portion of the lens posterior pole. Previous studies had used 20 MHz ultrasound to observe the posterior capsule of the lens[22-23], Tabatabaei et al[23]found 93%sensitivity and 86% specificity for the 20 MHz probe to detect a posterior capsule tear of any size. Kucukevcilioglu et al[24]reported one case with 1.0 mm posterior capsule irregularity using 35 MHz UBM, they emphasized that 35 MHz UBM was equipped with 70 μm of axial-lateral resolution and penetration of 7.0 to 8.0 mm probe, as a result, it could provide more detailed evaluation of the zonule and ciliary body because of its deeper penetration than 50 MHz UBM and higher resolution than 20 MHz ultrasound. With a penetration of 9.0 mm and 50 μm of axial-lateral resolution, 25 MHz UBM is another novel and practical ultrasonic diagnostic tool for the integrity of posterior lens capsule.
Other anterior segment inspection modalities, such as the Pentacam, Orbscan II, and AS-OCT, can also obtain anterior segment images, but they cannot display an ideal lens image.The Pentacam can be used in nuclear cataract grading and the preoperative evaluation of the lens nucleus density in the case of mydriasis[25-26]. Kim et al[27]showed that although the Pentacam can effectively measure lens nucleus density, it is dif ficult to measure the posterior cortex and posterior capsule,even if the pupil is fully dilated. The use of 25 MHz UBM is not affected by pupil size and refractive media opacity, and it showed the lens opacity and site more clearly than 50 MHz UBM and other anterior segment inspection modalities.
In conclusion, compared with 50 MHz UBM, 25 MHz UBM had a greater advantage in showing the complete morphology of the lens. It can provide reliable imaging of the lens and its related diseases and has a high application value for ophthalmology. The use of 25 MHz UBM plays an irreplaceable role in the study of lens diseases. And a combination of these two frequencies may be the best method to obtain an objective imaging diagnosis of the anterior segment tissue in clinical practice.
Conflicts of Interest: Shi MY,None;Han X,None;Zhang JS,None;Yan QC,None.
REFERENCES
1 Timoney PJ, Breathnach CS. Allvar Gullstrand and the slit lamp 1911.Ir J Med Sci2013;182(2):301-305.
2 Utine CA, Altin F, Cakir H, Perente I. Comparison of anterior chamber depth measurements taken with the Pentacam, Orbscan IIz and IOLMaster in myopic and emmetropic eyes.Acta Ophthalmol2009;87(4):386-391.
3 Whang WJ, Byun YS, Joo CK. Comparison of refractive outcomes using five devices for the assessment of preoperative corneal power.Clin Exp Ophthalmol2012;40(5):425-432.
4 Nassiri N, Sheibani K, Sa fiS, Nassiri S, Ziaee A, Haji F, Mehravaran S,Nassiri N. Central corneal thickness in highly myopic eyes: inter-device agreement of ultrasonic pachymetry, pentacam and orbscan II before and after photorefractive keratectomy.J Ophthalmic Vis Res2014;9(1):14-21.
5 Pavlin CJ, Sherar MD, Foster FS. Subsurface ultrasound microscopic imaging of the intact eye.Ophthalmology1990;97(2):244-250.
6 Sherar MD, Starkoski BG, Taylor WB, Foster FS. A 100 MHz B-scan ultrasound backscatter microscope.Ultrason Imaging1989;11(2):95-105.
7 Foster FS, Pavlin CJ, Harasiewicz KA, Christopher DA, Turnbull DH. Advances in ultrasound biomicroscopy.Ultrasound Med Biol2000;26(1):1-27.
8 Pavlin CJ, Harasiewicz K, Sherar MD, Foster FS. Clinical use of ultrasound biomicroscopy.Ophthalmology1991;98(3):287-295.
9 Pavlin CJ, McWhae JA, McGowan HD, Foster FS. Ultrasound biomicroscopy of anterior segment tumors.Ophthalmology1992;99(8):1220-1228.
10 Elfiky M, Saad H, Elseht R, Selima A. Role of ultrasound biomicroscopy in the planning for secondary implantation of intra ocular lens in aphakia.Int Ophthalmol2016;36(3):391-400.
11 Ramasubramanian V, Glasser A. Prediction of accommodative optical response in prepresbyopic subjects using ultrasound biomicroscopy.J Cataract Refract Surg2015;41(5):964-980.
12 Estremadoyro DLT, Danilo M. Ultrasound biomicroscopy enhances ophthalmic imaging applications.Ophthalmology Times2014;39(12):14-15.13 Silverman RH. High-resolution ultrasound imaging of the eye-a review.Clin Exp Ophthalmol2009;37(1):54-67.
14 Zhao Y, Wei W, Zhang CN. Comparison of anterior segment parameters with Lenstar 900 and Sirius system.Guoji Yanke Zazhi (Int Eye Sci)2014;14(7):1250-1252.
15 Sihota R, Vashisht P, Sharma A, Chakraborty S, Gupta V, Pandey RM.Anterior segment optical coherence tomography characteristics in an Asian population.J Glaucoma2012;21(3):180-185.
16 Chiranjib M, Chin TY. Comparison of ocular biometry and corneal curvature among malaysian emmetropes and myopes.Indian Journal of Scientific Research2015;6(1):1-9.
17 Paunksnis A, Kurakiene S. Maciulis A, Kopustinskas A, Paunksniene M. Ultrasound quantitative evaluation of human eye cataract.Informatica2007;18(2):267-278.
18 Chylack LT Jr, Wolfe JK, Singer DM, Leske MC, Bullimore MA,Bailey IL, Friend J, McCarthy D, Wu SY. The lens opacities classification system III. The longitudinal study of cataract study group.Arch Ophthalmol1993;111(6):831-836.
19 Karbassi M, Khu PM, Singer DM, Chylack LT Jr. Evaluation of lens opacities classification system III applied at the slitlamp.Optom Vis Sci1993;70(11):923-928.
20 Tan AC, Loon SC, Choi H, Thean L. Lens opacities classification system III: cataract grading variability between junior and senior staff at a Singapore hospital.J Cataract Refract Surg2008;34(11):1948-1952.
21 Stachs O, Martin H, Behrend D, Schmitz KP, Guthoff R. Threedimensional ultrasound biomicroscopy, environmental and conventional scanning electron microscopy investigations of the human zonular ciliaris for numerical modelling of accommodation.Graefes Arch Clin Exp Ophthalmol2006;244(7): 836-844.
22 Nguyen TN, Mansour M, Deschenes J, Lindley S. Visualization of posterior lens capsule integrity by 20-MHz ultrasound probe in ocular trauma.Am J Ophthalmol2003;136(4):754-755.
23 Tabatabaei A, Kiarudi MY, Ghassemi F, Moghimi S, Mansouri M,Mirshahi A, Kheirkhah A. Evaluation of posterior lens capsule by 20-MHz ultrasound probe in traumatic cataract.Am J Ophthalmol2012;153(1):51-54
24 Kucukevcilioglu M, Hurmeric V, Ceylan OM. Preoperative detection of posterior capsule tear with ultrasound biomicroscopy in traumatic cataract.J Cataract Refract Surg2013;39(2):289-291.
25 Magalhaes FP, Costa EF, Cariello AJ, Rodrigues EB, Hofling-Lima AL. Comparative analysis of the nuclear lens opalescence by the lens opacities classification system III with nuclear density values provided by Oculus Pentacam: a cross-section study using pentacam nucleus staging software.Arq Bras Oftalmol2011;74(2):110-113.
26 Gupta M, Ram J, Jain A, Sukhija J, Chaudhary M. Correlation of nuclear density using the lens opacity classification system III versus Scheimpflug imaging with phacoemulsification parameters.J Cataract Refract Surg2013;39(12):1818-1823.
27 Kim JS, Chung SH, Joo CK. Clinical application of a Scheimpflug system for lens density measurements in phacoemulsification.J Cataract Refract Surg2009;35(7):1204-1209.
Correspondence to:Qi-Chang Yan. Department of Ophthalmology, the Fourth Affiliated Hospital of China Medical University, No.11 Xinhua Road, Heping District, Shenyang 110005, Liaoning Province, China. cmu4h-yqc@126.com
Received:2017-03-18 Accepted: 2017-04-25
Abstract ● AlM: To compare the results of 25 MHz and 50 MHz ultrasound biomicroscopy (UBM) regarding the image characteristics of the lens and its related diseases and to discuss the application value of 25 MHz UBM in ophthalmology.● METHODS: A total of 302 patients (455 eyes) were included in this study from November 2014 to May 2015.Patient ages ranged from 5 to 89y (mean±SD: 61.0±17.7y).Different cross-sectional images of the lens were collected to compare and analyze the image characteristics and anterior segment parameters using 25 MHz and 50 MHz UBM in axial and longitudinal scanning modes, respectively. SPSS 19.0 for Windows, paired t-tests and B&A plot analysis were used for data analysis, and a value of P<0.05 was considered statistically significant.● RESULTS: The 25 MHz UBM images displayed the lens shape more clearly than 50 MHz UBM images. Particularly for cataracts, the whole opacity of the lens was shown by 25 MHz UBM, but 50 MHz UBM only showed part of the lens. The means of the anterior segment parameters obtained using 25 MHz and 50 MHz UBM were as follows:central corneal thickness: 0.55±0.03 and 0.51±0.04 mm,respectively; central anterior chamber depth: 2.48±0.54 and 2.56±0.56 mm, respectively; and central lens thickness: 4.26±0.62 and 4.15±0.56 mm, respectively. A statistically significant difference was found between the results obtained with 25 MHz UBM and those obtained with 50 MHz UBM. The two devices had a good agreement in measuring the anterior segment parameters.● CONCLUSlON: The 25 MHz UBM had an obvious advantage in showing the lens shape. lt can provide reliable imaging of the lens and its related diseases and has a high application value for ophthalmology.
● KEYWORDS:25 MHz ultrasound biomicroscopy; 50 MHz ultrasound biomicroscopy; lens diseases
DOl:10.18240/ijo.2018.07.13
Citation:Shi MY, Han X, Zhang JS, Yan QC. Comparison of 25 MHz and 50 MHz ultrasound biomicroscopy for imaging of the lens and its related diseases. Int J Ophthalmol 2018;11(7):1152-1157