Table 1 Descriptive analysis of sociodemographic variables and variables of interest pre-phacoemulsification
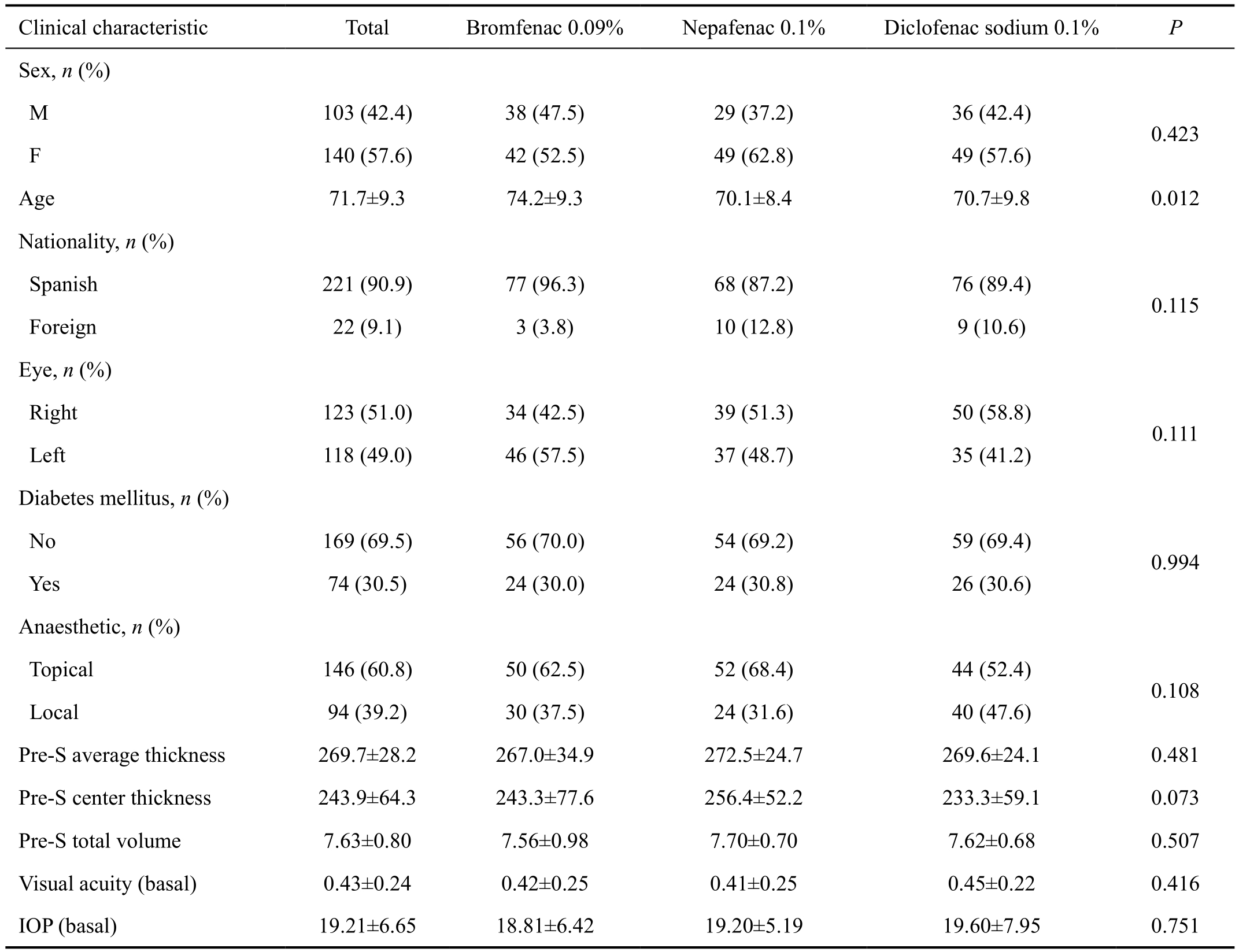
Pre-S: Pre-surgery; IOP: Intraocular pressure. Patients treated with bromfenac 0.09%, nepafenac 0.1% and diclofenac sodium 0.1% eye drops.
Ana María Chinchurreta Capote1, Mercedes Lorenzo Soto1, Francisco Rivas Ruiz2,3, Enrique Caso Peláez2,3, Alicia García Vazquez1, Group OftaCosta1, Antonio Ramos Suárez1
1Ophthalmology Service, Health Agency Costa del Sol,Marbella, Málaga 29603, Spain
2Research Unit, Health Agency Costa del Sol Marbella,Málaga 29603, Spain
3National Research Network of Health Services in Chronic Diseases (REDISSEC), Madrid 28029, Spain
Cystoid macular edema (CME) is the most common cause of vision loss after uncomplicated cataract surgery, has an incidence of 0.1%, and there is no total consensus about its prophylaxis and treatment[1-2]. This pathology is associated with the blood-retinal barrier disruption induced by prostaglandins(PG) and other in flammatory mediators[3].
The currently available topical non-steroidal anti-in flammatory drugs (NSAIDs) for prevention and management of noninfectious ocular inflammation and CME in USA and Europe include bromfenac, indomethacin, diclofenac, flurbiprofen, ketorolac tromethamine and nepafenac.
These drugs have been proven to be a safe and effective alternative to corticosteroids in the topical prevention and management of CME. Several studies assessed and compared the effectiveness of each of those drugs; however, there are no relevant studies comparing post-phacoemulsification effectiveness and tolerability of diclofenac sodium, bromfenac and nepafenac[4-6].
Clinicians have examined the effectiveness of postphacoemulsification CME control with NSAIDs after regulatory approval. Miyake et al[7]found that diclofenac was more effective in preventing CME than a topical corticosteroid eyedrop, fluorometholone. Indomethacin, among NSAIDs,has been used to prevent CME after cataract surgery and has good intraocular bioavailability[8]. Miyake et al[9]found that nepafenac 0.1% was more effective in preventing CME following cataract surgery than fluorometholone 0.1%.Wang et al[10]showed that bromfenac 0.1% was superior to both fluorometholone and dexamethasone in preventing CME following phaco emulsification. In an animal model,Bucolo et al[11]evaluated the effects of topical indomethacin,bromfenac and nepafenac on lipopolysaccharide-induced ocular inflammation and found that only indomethacin was able to prevent retinal vascular leakage in rats.
Macular thickness increases in 27% to 41% of eyes undergoing phacoemulsification. Many studies assess the action of NSAIDs on the macular volume regarding postphacoemulsification CME prevention. Most of them conclude that even though the little increase of the macular thickness following uncomplicated cataract surgery is not clinically significant, the use of those drugs would be advisable after such operation to ensure an excellent final visual acuity.However, there is no evidence about which of the NSAIDs could be the most effective[12-13].
We compared effectiveness of diclofenac sodium 0.1%, bromfenac 0.09% and nepafenac 0.1% in post-phacoemulsification CME prevention, by evaluating the macular volume using optical coherence tomography (OCT), and we examined the tolerability by ophthalmologic examination and a patient reported outcome questionnaire.
Group sequential observational comparative study of the effectiveness, tolerability and safety in the use of postphacoemulsification anti-in flammatory topical drugs. The study population consisted of patients on the waiting list for cataract surgery by the Costal del Sol Health Agency and without having any exclusion criteria, underwent phacoemulsification surgery and intraocular lens implantation in the posterior chamber together with post-surgery topical anti-in flammatory treatment. The study duration was 6mo of post-operative follow up. We enrolled patients from June to December 2015.We used the following exclusion criteria: history of allergic reaction to topical NSAIDs, history of weight loss, corneal erosion, ulcer or perforation, history of retinal disease (diabetic macular edema, proliferative diabetic retinopathy, age-related macular degeneration and post central and branch retinal vein occlusion edema), prior uveitis, intraocular surgery or advanced glaucoma.
As part of the clinical history at the preoperative initial visit we recorded the following: the eye operated, type of ocular anaesthetic, and history of diabetes mellitus. The eye examination included: best corrected visual acuity (BCVA),intraocular pressure (IOP), biomicroscopy (BM), ocular fundus(OF) and OCT using Topcon three-dimensional OCT 2000(Topcon Medical Systems, Inc., Oakland, NJ, USA). The latter assessed the average macular thickness in microns (AT), the central foveal thickness in microns (CT) and the total macular volume in cubic millimeter (TV).
After surgery, we separated treatment groups into intervals of 2mo for topical treatment with diclofenac sodium 0.1% (for the first two months of the study), bromfenac 0.09% (for the following two months of the study) and nepafenac 0.1% (for the last two months of the study), all of them combined with an antibiotic and a steroid. Patients were instructed to instill a drop of diclofenac sodium 0.1% in the operated eye four times per day, a drop of bromfenac 0.09% twice a day, and a drop of nepafenac 0.1% three times a day. They started the topical treatment with NSAID on the first post-operation day (day 1),and continued for three weeks for diclofenac sodium 0.1%and nepafenac 0.1%, and two weeks for bromfenac 0.09%. All patients received topical tobramycin 0.03% (four times daily),starting 3d before the surgery and finishing one week after it,and topical prednisolone 1% (after the phacoemulsification)with the following administration regimen: every hour for the first 24h, 4 times daily for the first week, 3 times daily for the second week, twice daily during the third week, and once daily the fourth week.
The postoperative examination of the patient was carried out on day 1 (visit 1), at week 3 (visit 2), and 2mo after phacoemulsification (visit 3). OCT was performed before surgery, at week 3 and 2mo after surgery. At visit 1 BCVA, IOP and BM were assessed. At visit 2 BCVA, IOP, BM, OF and the OCT were assessed. At visit 3 OCT imaging was performed and patients filled in the questionnaire about their satisfaction with their medication treatment. Every item in it was scored from 1 (minimum) to 5 (maximum). Items are shown in Table 4. During the whole survey all postoperative problems were considered. The study protocol was reviewed by the central internal review board for the investigational site, and the study was conducted in accordance with the principles stated in the Declaration of Helsinki. Written informed consent was obtained from all patients before initiation of study specific procedures.
Statistical AnalysisDescriptive analysis was conducted with measures of central tendency and dispersion for quantitative variables, and distribution of frequencies for the qualitative ones. In the comparison of the three treatment groups, the onefactor ANOVA test was used for the quantitative variables result, including 95% confidence intervals (95%CI) for mean values, and Chi-square test was used for the qualitative variables result. Statistical significance level was set at P<0.05 and statistical analysis was performed using SPSS 19.0(SPSS®, Chicago, IL, USA).
A total of 243 patients were studied, of which 85 (35%)were treated with diclofenac sodium 0.1%, forming Group A; 80 (32.9%) were treated with bromfenac 0.09%, forming Group B; and 78 (32.1%) were treated with nepafenac 0.1%,forming Group C. Median age was 71.7 years old (SD 9.3),it was different in each of the three groups (P=0.012) and higher in the bromfenac 0.09% group (74.2, SD 9.3). There were no differences among groups in the rest of pretreatment sociodemographic variables. Of the participants, 57.6% werewomen, and 90.9% had Spanish nationality. The operated eye was the right one in 51% of patients, 30.5% had diabetes mellitus, and topical anaesthetic (60.8%) was the most frequent type (Table 1).
Table 1 Descriptive analysis of sociodemographic variables and variables of interest pre-phacoemulsification
Pre-S: Pre-surgery; IOP: Intraocular pressure. Patients treated with bromfenac 0.09%, nepafenac 0.1% and diclofenac sodium 0.1% eye drops.
In the assessment of pre-surgery indicators and the 3-week and 2-month monitoring, significant differences in the CT value were found among groups. Thus, at the 3wk monitoring, CT was reduced in the bromfenac group by -21.3 mm3(95%CI:-40.7 -1.9), versus diclofenac sodium (-1.3; 95%CI: -13.3-10.7), and nepafenac, where it increased 6.4 mm3(6.4; 95%CI:-7.2 -20), for a P value of 0.037. At the 2mo assessment, the CT in the bromfenac group was reduced by -35.4 (95%CI: -61.5-9.3), versus nepafenac (5.3; 95%CI: -9.3 -19.9) and diclofenac(-11.5; 95%CI: -24.4-1.5), for a P value of 0.015 (Table 2).
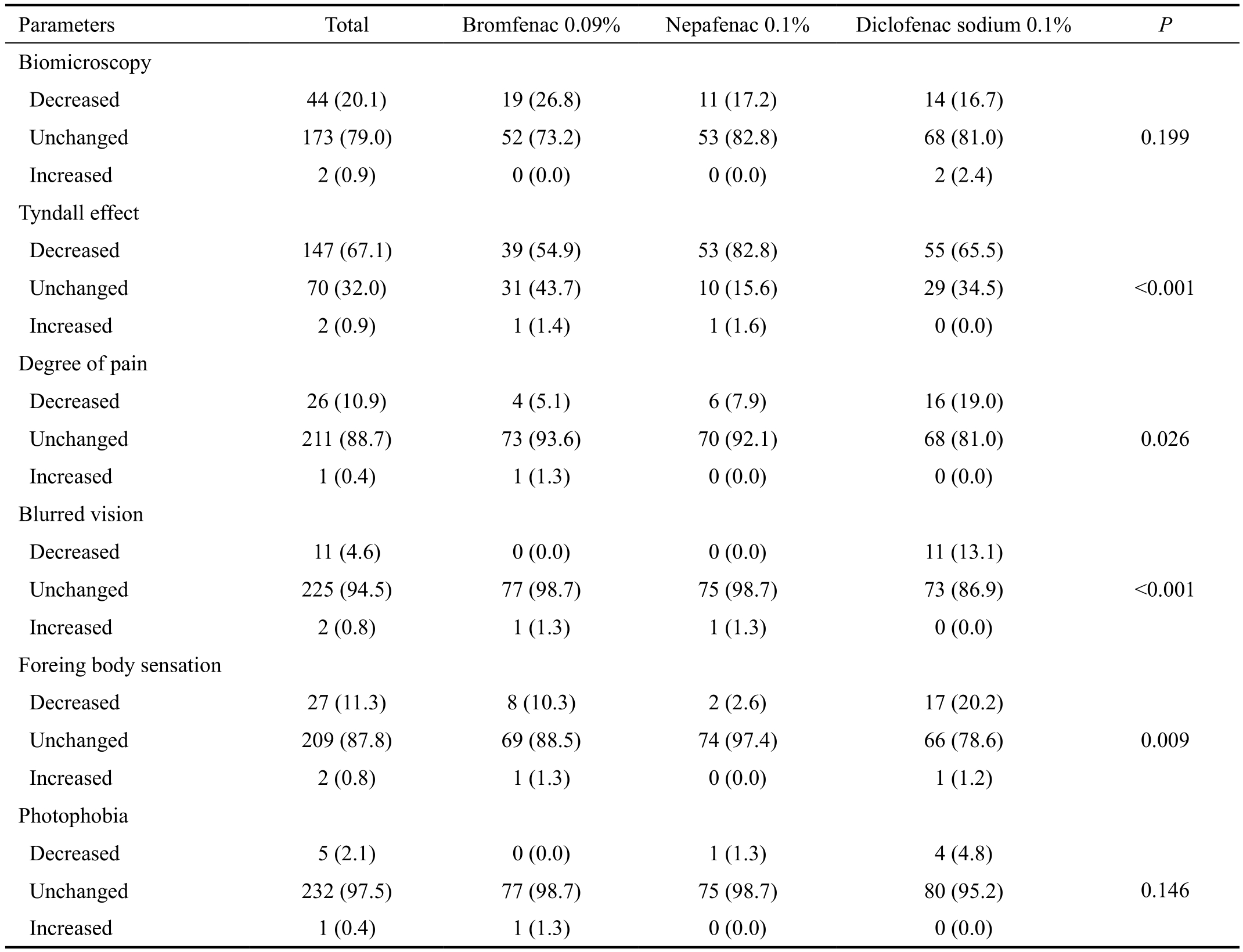
In the assessment of qualitative indicators, significant differences were found among groups (P<0.001) for the Tyndall effect,since such effect was reduced in 82.8% of patients of the nepafenac 0.1% group, while in the diclofenac sodium 0.1%group reduction was achieved in 65.5% of patients, and in 54.9% of patients of the bromfenac 0.09% group. Also notable differences (P=0.026) were observed among groups in the degree of pain, which decreased by 19% in patients of diclofenac sodium 0.1%; in the blurred vision (P<0.001), with a reduction of 13.1% in the diclofenac group; and the foreign body sensation (P=0.009) was reduced in 20.2% also in the diclofenac group (Table 3).
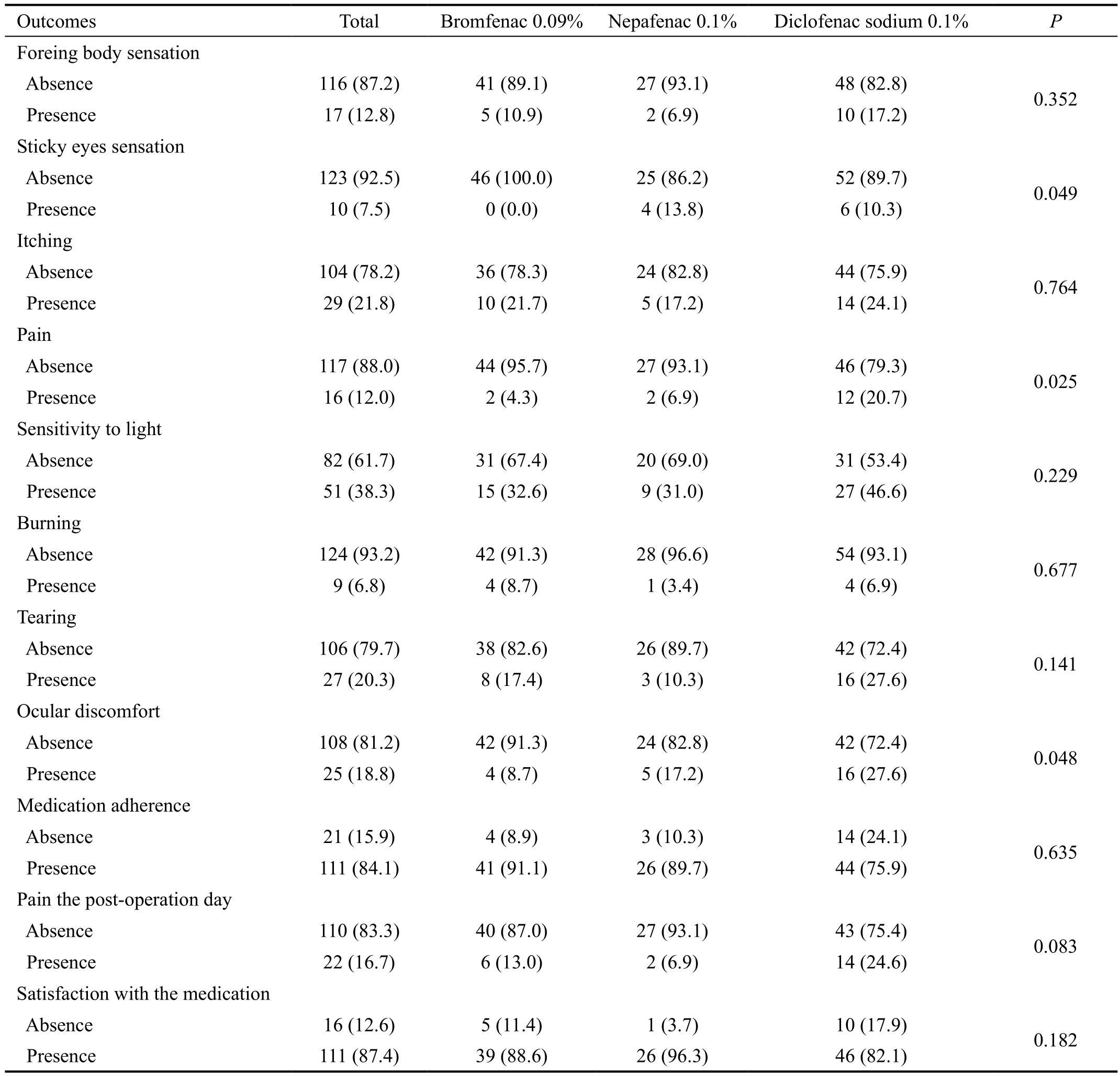
Finally, postsurgical satisfaction questionnaire was completed by a total of 133 patients, of which 46 (34.6%) were treated with bromfenac 0.09%, 29 (21.8%) with nepafenac 0.1%and 58 (43.6%) with diclofenac sodium 0.1%. Globally,84.1% had a correct medication adherence, 16.7% reported pain the postoperation day and 87.4% were satis fied with the medication. There were significant differences among groups for the variable of sticky eyes sensation (P=0.049), since that condition was present in 13.8% of the nepafenac 0.1% group,versus 10.3% in the diclofenac sodium 0.1%, while absent in all patients of the bromfenac 0.09% group. Likewise, there were important differences for the pain variable (P=0.025),since 20.7% of patients from the diclofenac sodium 0.1%reported present pain, versus 6.9% of the nepafenac 0.1%group and 4.3% of the bromfenac 0.09% group. Differences were also found for the ocular discomfort variable (P=0.048),with discomfort reported by 27.6% of patients in the diclofenac sodium 0.1% group, by 17.2% of patients treated with nepafenac 0.1%, and 8.7% from the bromfenac 0.09% group(Table 4).
Table 2 Evolution of quantitative indicators of macular thickness by OCT in patients with ocular topical treatment of bromfenac 0.09%, nepafenac 0.1% and diclofenac sodium 0.1%
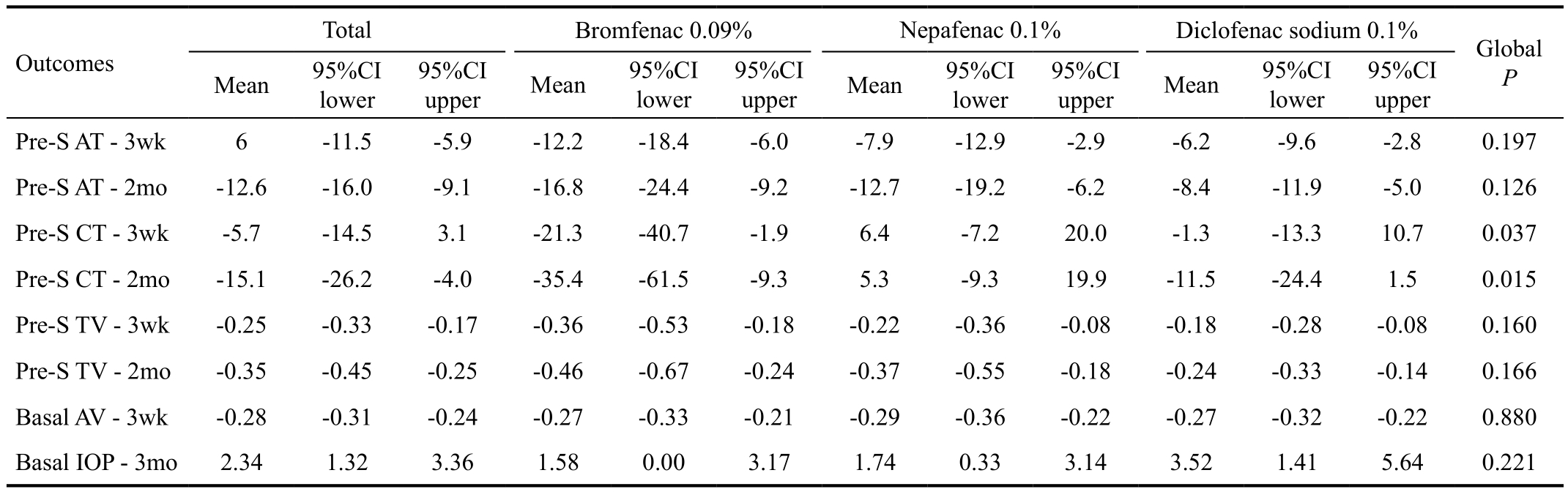
It shows mean changes among basal values and monitoring of each indicator. AT: Average macular thickness in microns; CT: Central foveal thickness in microns; TV: Total macular volume in mm3; Pre-S: Pre-surgery; IOP: Intraocular pressure; AV: Visual acuity; CI: Con fidence interval.
Table 3 Evolution of qualitative indicators after ophthalmologic examination of the study patients according with their treatment n (%)
We found bromfenac is the most effective for the CME prevention and nepafenac was the least effective. We found nepafenac was the most effective and bromfenac the least in reducing in flammation (through the Tyndall effect).
Through our patient reported outcome survey, patientsreported diclofenac achieved the highest reduction of pain,and bromfenac, the lowest; diclofenac reduced the blurred vision and foreign body sensation the most. No patients using bromfenac reported a sticky eyes sensation. The drug which caused the most ocular discomfort was diclofenac,and bromfenac was the one which caused the least. The highest medication adherence was performed by patients in the bromfenac group, and the lowest, by the diclofenac one.The highest satisfaction was reported by the group that used nepafenac, and the lowest by the diclofenac group.
Table 4 Comparative chart of the post-surgery satisfaction questionnaire results, according to drug used n (%)
Our study has limitations in the satisfaction questionnaire completion, as of the 243 participants, just over half of them answered it. Among the main reasons of that low response rate are mostly forgetting to complete it, losing the questionnaire form, and having no relatives to help them.
Multivariate analysis has not been carried out for all the described outcome variables: evolution of indicators, qualitative indicators, and satisfaction indicators due to insuf ficient sample power. Only multivariate linear regression analysis has been performed to adjust for age, and pre-surgery CT (which are the two variables below P<0.1 in bivariate analysis) for both the outcome variable of the CT follow up at 3wk and 2mo, and in both cases significant differences remain between treatment groups (results not described).
Therefore, this is an observational comparative study, which assesses the effectiveness of the treatment in clinical practice.Both the pre-surgery and post-surgery assessments were carried out by the same examiner. The surgery, the post-surgical examination and the OCT were performed by physicians with more than 10y of experience in those procedures.
Cataract surgery is one of the surgical techniques more frequently practiced in developed countries. CME is the most frequent cause of visual loss after phacoemulsification. CME is normally a subclinical and self-limited process, but in a small group of patients it turns into a chronic process with permanent loss of visual acuity. Its appearance can occur after a few weeks post-surgery to months later[14].
Many studies report the higher efficacy of topical NSAIDs in preventing post-cataract surgery CME compared to topical corticosteroids. However, studies trying to find the best post-phacoemulsification NSAID do not provide consistent differences among them. In that sense, in the literature there are no relevant clinical comparative studies about the capacity of diclofenac sodium 0.1%, nepafenac 0.1% and bromfenac 0.09% to control post-cataract surgery inflammation, nor comparative studies about the patient’s subjective satisfaction with those NSAIDs or their possible adverse effects[5].
Kessel et al[4]perform a systematic review of articles published from 1996 comparing topical corticoids’ effectiveness versus NSAIDs to control post cataract phacoemulsification CME.Their conclusion is that NSAIDs are more effective for that purpose with a high level of evidence. Nevertheless, no differences were found in the final VA and the number of adverse effects, except for the increase of IOP in patients treated with corticoids. They did not include studies analyzing the efficacy of the different types of NSAIDs by separate.
We do not show any clinically important difference regarding visual acuity in the NSAIDs we studied.
Russo et al[15]conclude that the combined use of NSAIDs and topical corticosteroids has synergic effect in controlling postcataract surgery CME. However, the systematic use in patients with low risk of CME is questionable, given the CME low incidence among them. Shoss et al[16]conclude that, although topical NSAIDs reduce post-cataract surgery CME incidence,this incidence is very low, and their systematic is not recommended for uncomplicated surgeries or for patients with corneal pathology. Combined use of corticosteroids with topical NSAIDs could reduce the latter’s damaging effect on the cornea.Topical NSAIDs may have harmful effects on the cornea, like super ficial punctate keratopathy, in filtrates, or corneal melting.In our study we did not detect any corneal adverse events.
Schoenberger et al[17]observe that there is no evidence of which NSAID is the most effective, but report flurbiprofen is less effective. We will need further investigation to more conclusively demonstrate which of the three NSAIDs would be more safe and effective after cataract surgery.
Nevertheless, some investigators have reported superiority of bromfenac and nepafenac. Thus, Warren et al[18]studied the effect of the combined use of topical NSAIDs with intravitreal corticosteroids (triamcinolone) and anti-VEGF (bevacizumab)in the control of chronic pseudophakic CME and compared diclofenac, ketorolac, nepafenac and bromfenac. Using NSAIDs together with corticosteroids and anti-VEGF seemed to increase effectiveness, but only bromfenac and nepafenac were effective compared to placebo.
Jones et al[19]come to the conclusion that the topical use of bromfenac 0.09% twice a day is superior to placebo in controlling post-cataract surgery intraocular inflammation.Silverstein et al[20], concluded as well, that bromfenac 0.07%dosed once daily was clinically effective in achieving zero-totrace anterior chamber cell severity after cataract surgery and superior to placebo in all anterior chamber cell severity and in flammation outcome measures.
The results of our study show that bromfenac 0.09% obtains a greater reduction of the retinal thickness values, both at postphacoemulsification 3-week and 2-month OCT measurements.Patient’s subjective satisfaction was highest with bromfenac 0.09%. Regarding safety, we record no important adverse effect with any of the three drugs during the follow up period.We cannot conclude which of the three drugs should be preferentially used after cataract surgery, although we found bromfenac 0.09% most effectively reduced foveal thickness.Also, patient’s satisfaction level was highest with bromfenac 0.09%. The increased cost of bromfenac 0.09% compared to diclofenac 0.1% needs to be assessed with the clinical significance of its increased efficacy.
We plan to perform further investigation of postphacoemulsification NSAIDs by including a fourth treatment arm of corticosteroids alone as well as investigate a new commercial preparation of nepafenac 0.3%.
The authors would like to acknowledge the exceptional efforts in the development of the research to the group OftaCosta.
Group authors’ names: Saturnino Gismero Moreno, Jose María Requena Jiménez, Juan Miguel Nieto Martín, Fernando García Marín, Sergio Del Río Fernández, Aniceto Jaime Corcelles Ledesma, Susana García Marcet, Carmen Del Pozo Rodríguez,Encarnación Alijo Serrano, Elena Barco Moreno, Antonio Alberte González, María del Mar Brieba López del Amo,Francisco Villalobos Loriguillo, Yolanda Fernández Barrientos,Ana Belén González Escobar, Francisco Javier Barrero Sojo,Ainsa Ibáñez García, Yolanda Sánchez García, Cándido Ruiz Rincón, Irene Lara Malpartida, María Dolores Salazar.
Conflicts of Interest: Chinchurreta Capote AM,None;Lorenzo Soto M,None;Rivas Ruiz F,None;Caso Peláez E,None;García Vázquez A,None;Group OftaCosta,None;Ramos Suárez A,None.
REFERENCES
1 Packer M, Lowe J, Fine H. Incidence of acute postoperative cystoid macular edema in clinical practice.J Cataract Refract Surg2012;38(12):2108-2111.
2 Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema.Curr Opin Ophthalmol2012;23(1):26-32.
3 Semeraro F, Russo A, Gambicorti E, Duse S, Morescalchi F, Vezzoli S, Costagliola C. Efficacy and vitreous levels of topical NSAIDs.Expert Opin Drug Deliv2015;12(11):1767-1782.
4 Kessel L, Tendal B, Jørgensen KJ, Erngaard D, Flesner P, Andresen JL,Hjortdal J. Post-cataract prevention of in flammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: a systematic review.Ophthalmology2014;121(10):1915-1924.
5 Duan P, Liu Y, Li J. The comparative efficacy and safety of topical nonsteroidal anti-in flammatory drugs for the treatment of anterior chamber in flammation after cataract surgery: a systematic review and network meta-analysis.Graefes Arch Clin Exp Ophthalmol2017;255(4):639-649.
6 McCafferty S, Harris A, Kew C, Kassm T, Lane L, Levine J, Raven M. Pseudophakic cystoid macular edema prevention and risk factors;prospective study with adjunctive once daily topical nepafenac 0.3%versus placebo.BMC Ophthalmol2017;17(1):16.
7 Miyake K, Nishimura K, Harino S, Ota I, Asano S, Kondo N, Miyake S. The effect of topical diclofenac on choroidal blood flow in early postoperative pseudophakias with regard to cystoid macular edema formation.Invest Ophthalmol Vis Sci2007;48(12):5647-5652.
8 Bucolo C, Melilli B, Piazza C, Zurria M, Drago F. Ocular pharmacokinetics profile of different indomethacin topical formulations.J Ocul Pharmacol Ther2011;27(6):571-576.
9 Miyake K, Ota I, Miyake G, Numaga J. Nepafenac 0.1% versus fluorometholone 0.1% for preventing cystoid macular edema after cataract surgery.J Cataract Refract Surg2011;37(9):1581-1588.
10 Wang QW, Yao K, Xu W, Chen PQ, Shentu XC, Xie X, Weng Y, Zhang L, Jin CF, Wu W, Zhu YN, Yu YH. Bromfenac sodium 0.1%, fluorometholone 0.1% and dexamethasone 0.1% for control of ocular inflammation and prevention of cystoid macular edema after phacoemulsification.Ophthalmologica2013;229(4):187-194.
11 Bucolo C, Marrazzo G, Platania CB, Romano GL, Drago F, Salomone S. Effects of topical indomethacin, bromfenac and nepafenac on lipopolysaccharide-induced ocular inflammation.J Pharm Pharmacol2014; 66(7):954-60.
12 Chu CJ, Johnston RL, Buscombe C, Sallam AB, Mohamed Q, Yang YC. Risk factors and incidence of macular edema after cataract surgery.Ophthalmology2016;123(2):316-323.
13 Hoffman RS, Braga-Mele R, Donaldson K, Emerick G, Henderson B,Kahook M, Mamalis N, Miller KM, Realini T, Shorstein NH, Stiverson RK, Wirostko B. Cataract surgery and nonsteroidal anti-inflammatory drugs.J Cataract Refract Surg2016;42(9):1368-1379.
14 Corrêa EP, Oliveira LF, Serracarbassa PD, Oshima A, Sousa e Castro EF. Evaluation of macular edema after uncomplicated phacoemulsification surgery with implantation of intraocular lens by spectral domain optical coherence tomography.Arq Bras Oftalmol2013;76(6):357-362.
15 Russo A, Costagliola C, Delcassi L, Parmeggiani F, Romano MR,Dell´Omo R, Semeraro F. Topical nonsteroidal anti-in flammatory drugs for macular edema.Mediators In flamm2013;2013:476525.
16 Shoss BL, Tsai LM. Postoperative care in cataract surgery.Curr Opin Ophthalmol2013;24(1):66-73.
17 Schoenberger SD, Kim SJ. Nonsteroidal anti-in flammatory drugs for retinal disease.Int J In flam2013;2013:281981.
18 Warren KA, Bahrani H, Fox JE. NSAIDs in combination therapy for the treatment of chronic pseudophakic cystoid macular edema.Retina2010;30(2):260-266.
19 Jones J, Francis P. Ophthalmic utility of topical bromfenac, a twicedaily nonsteroidal anti-inflammatory agent.Expert Opin Pharmacother2009;10(14):2379-2385.
20 Silverstein SM, Jackson MA, Goldberg DF, Muñoz M. The efficacy of bromfenac ophthalmic solution 0.07% dosed once daily in achieving zeroto-trace anterior chamber cell severity following cataract surgery.Clin Ophthalmol2014;8:965-972.
Correspondence to:Ana María Chinchurreta Capote. Health Agency Costa del Sol, Ophthalmology Service, Marbella,Málaga 29603, Spain. achinchu@gmail.com
Received:2017-10-25 Accepted: 2018-03-04
Abstract ● AlM: To compare the efficacy, tolerability and safety of bromfenac 0.09%, nepafenac 0.1% or diclofenac 0.1% for the prophylaxis of the cystoid macular edema (CME) after phacoemulsification.● METHODS: Group sequential observational comparative study. After phacoemulsification, patients received two months for topical treatment of either diclofenac sodium,bromfenac or nepafenac. All patients received concomitant topical tobramycin 0.3% and topical prednisolone 1%. We measured CME using optical coherence tomography (OCT)central foveal thickness, macular thickness and total macular volume.● RESULTS: We enrolled 243 patients from January to June 2015, and 35% received diclofenac, 32.9% bromfenac and 32.1% nepafenac. When we compared pre-operative to three weeks to two months, bromfenac was more effective in reducing foveal volume (21.3 and 35.4 mm3,respectively), compared with the diclofenac (1.3 and 11.5 mm3,respectively), and the nepafenac group, became more edematous 6.4 and 5.3, respectively. Totally 133 patients completed the post-surgical satisfaction questionnaire.Patients complained of eye stickiness in 13.8% whom we gave nepafenac, versus 10.3% whom we gave diclofenac sodium, and in 0 whom we gave bromfenac.● CONCLUSlON: Bromfenac is the best tolerated and is more effective than diclofenac and nepafenac in reducing CME after phacoemulsification.
● KEYWORDS:cystoid macular edema; bromfenac; diclofenac;nepafenac; phacoemulsification
DOl:10.18240/ijo.2018.07.22
Citation:Chinchurreta Capote AM, Lorenzo Soto M, Rivas Ruiz F,Caso Peláez E, García Vázquez A; Group OftaCosta, Ramos Suárez A.Comparative study of the efficacy and safety of bromfenac, nepafenac and diclofenac sodium for the prevention of cystoid macular edema after phacoemulsification. Int J Ophthalmol 2018;11(7):1210-1216