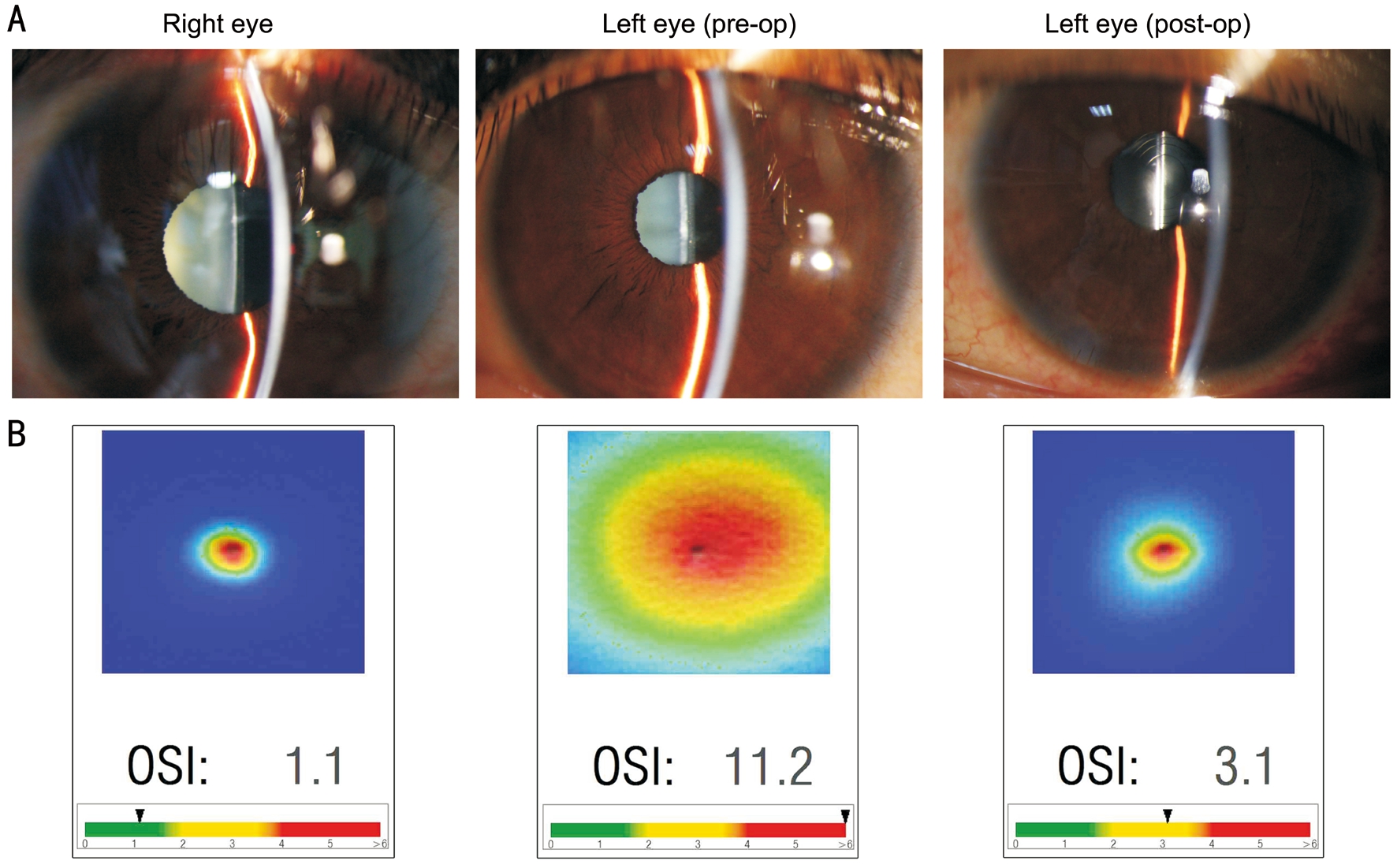
Figure 1 Anterior segment photography and visual quality A: Preoperative and postoperative slit-lamp photography; B: Objective optical quality analysis.
·Letter to the Editor·
Shu-Yang Chen, Chen Xie, Yang Wang, Ye Shen
Department of Ophthalmology, the First Affiliated Hospital,College of Medicine, Zhejiang University, Hangzhou 310003,Zhejiang Province, China
I am Dr. Ye Shen from the Department of Ophthalmology,the First Affiliated Hospital, College of Medicine,Zhejiang University, Hangzhou, China. I write to share my experience of full-vision maintenance in patient with extrahigh myopia from implantable collamer lens (ICL) to trifocal intraocular lens (IOL) implantation.
Visian ICL, a sulcus-placed posterior chamber phakic intraocular lens (PIOL) have been reported to provide effective, predictable and stable visual and refractive outcomes for moderate to high myopia[1-4]. An insufficient central or peripheral vault (the distance between the posterior surface of the ICL and the anterior surface of lens) increases the risk of cataract formation, the major postoperative complication as we reported[5-6]. Therefore, quite a few patients with young or middle age performed cataract surgery with monofocal IOL implantation to treat cataract after ICL implantation, while sacrificing the natural accommodation and increasing the spectacle dependence postoperatively.
The AT LISA tri 839MP has been proved to provide excellent visual acuity at far, intermediate, and near distance as the light is distributed into 3 foci: distance, intermediate, and near. The additions are +3.33 D (spectacle plane +2.5 D) for near (40 cm) and+1.66 D (spectacle plane +1.25 D) for intermediate (80 cm),respectively[7]. This case report described ICL explantation,phacoemulsification combining trifocal IOL implantation monocularly in a middle-aged patient, who presented with anterior subcapsular cataract in left eye after ICL implantation 2y.A 44-year-old female patient presented to our clinic complaining of gradually blurred vision in her left eye. The patient had history of bilateral ICL implantation to correct high myopia about two years ago (V4 Model; OD-ICM 12 mm/-22.5 D, OS-ICM 12 mm/-22 D). The patient demographics are listed in Table 1. Slit-lamp examination revealed the anterior subcapsular cataract in the left eye (Figure 1A). Ocular objective optical quality including modulation transfer function (MTF) cutoff frequency, objective scattering index (OSI), strehl ratio(SR) was obtained and assessed by Optical Quality Analysis System. A higher OSI value of 11.2 in the left eye indicated obvious increase of intraocular scattered light, which might cause a decreased visual quality (Figure 1B). Ultrasound biomicroscopy (UBM) revealed a small central vault of 0.16 mm,ICL in contact with the crystalline lens at the optic-haptic junction in the mid-peripheral areas in the left eye (Figure 2).The patient was scheduled to undergo ICL removal and phacoemulsification with a diffractive trifocal IOL (AT LISA tri 839MP) implantation in the left eye. The Haigis formula was found to be the most accurate in predicting postoperative refractive error in long eye[8-9], and was also a reliable choice in trifocal IOL implantation[10]. The Haigis formula was used to calculate the IOL power with the target refraction of -0.12 D,according to the values of keratometry, axial length (AL),and anterior chamber depth (ACD) obtained from the IOLMaster (IOL-Master 5000). A 3.0-mm clear corneal incision was created on the steep meridian of the corneal astigmatism.After the introduction of viscoelastic material into the anterior chamber, the proximal haptics of the ICL were dislocated,rotated 90 degrees clockwise, grasped with forceps, and extracted from the anterior chamber through the 3.0-mm incision. Routine phacoemulsification was performed and trifocal IOL implantation using the same 3.0-mm incision. No vision-threatening complications including intraocular pressure rise and posterior capsular opacity occurred during the follow-up.Visual acuity (far, intermediate and near) and visual performance(MTF, OSI, SR) of patient’s left eye were obviously improved postoperatively (Table 1). Postoperative uncorrected visual acuity (UVA) and corrected visual acuity (CVA) at 40 cm in the left eye achieved 20/25 and 20/20, respectively. Although the intermediate UVA at 1mo is 20/25, patient was still very satis fied with her visual outcome with no obvious discomfort during the follow up.
Figure 1 Anterior segment photography and visual quality A: Preoperative and postoperative slit-lamp photography; B: Objective optical quality analysis.
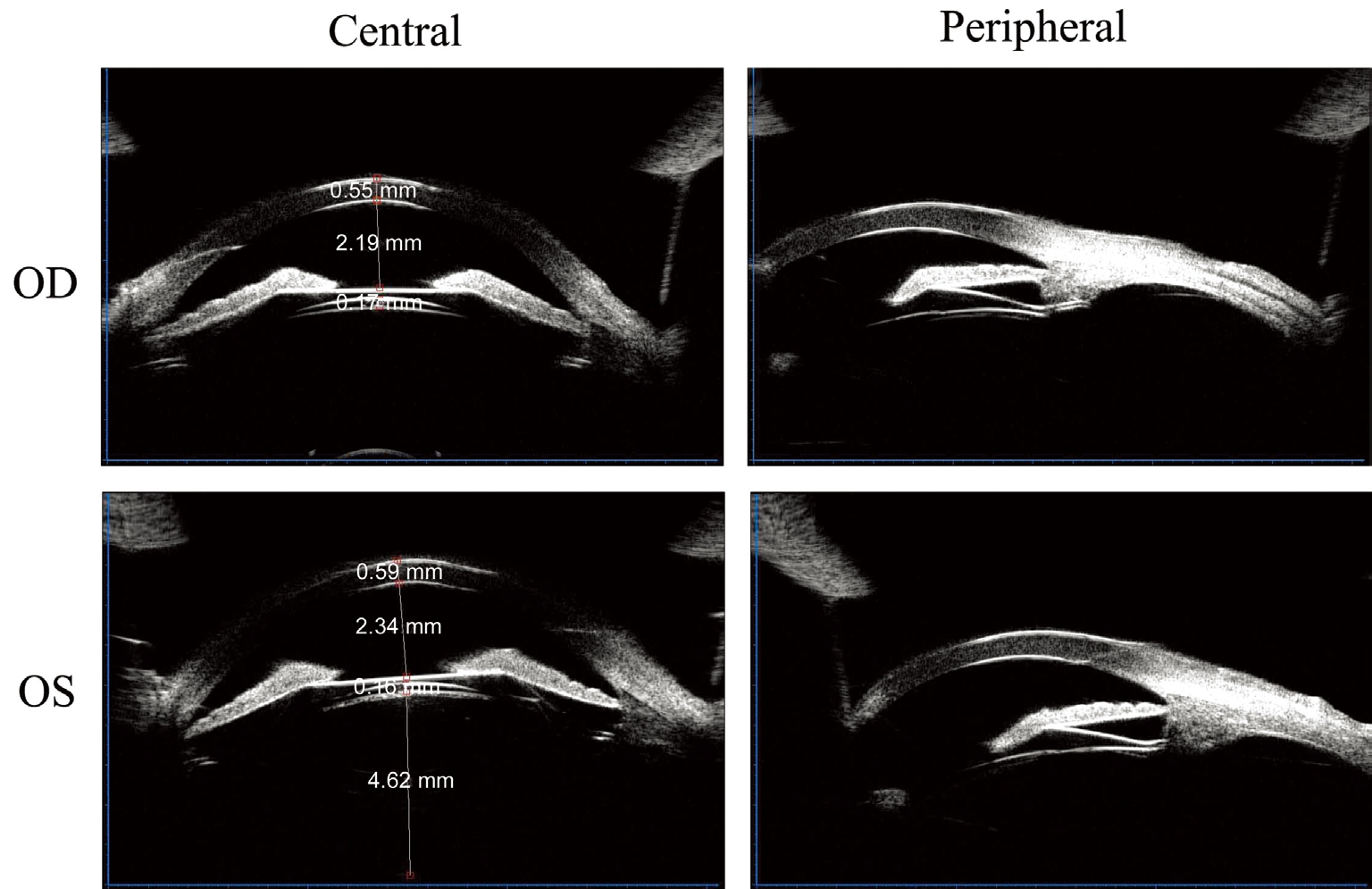
Figure 2 UBM examined the central and peripheral vault of ICL in the eyes.
The US Food and Drug Administration multicenter study[4]first reported that the incidences of anterior subcapsular opacities and developed nuclear opacities within 3y after ICL-V4 implantation were about 2.7% and 0.9%, respectively.Our long-term observation found no eyes with ICL-V4 in situ developed anterior subcapsular cataract with a mean peripheral vault of 0.253 mm within 2y, which indicated a peripheral vault greater than 0.25 mm is a safe parameter[6]. Besides the low vault, other risk factors for cataract formation included older age more than 45y, higher preoperative spherical equivalent (SE) greater than -14.00 D as mentioned by Maeng et al[11]. In this case reported, risk factors including 42-year-old,preoperative SE more than -18.00 D and a low ICL vault might contribute to the symptomatic anterior subcapsular opacities within early 2y after ICL-V4 implantation.
Recently, the first generation of diffractive trifocal IOL (the AT LISA tri 839MP) is designed to reduce spectacle dependence and improve subjective quality of vision in daily life activitiesafter cataract surgery. It has been proven to optimize the limitations of traditional multifocal IOLs, such as poor level of intermediate vision and photic phenomena[12-13]. Even though,we are unaware of any previous studies reported about trifocal IOL implantation in patient with posterior chamer PIOL and could not find a reference to it in a computerized research(database: PubMed).
Table 1 Preoperative and postoperative data of patient
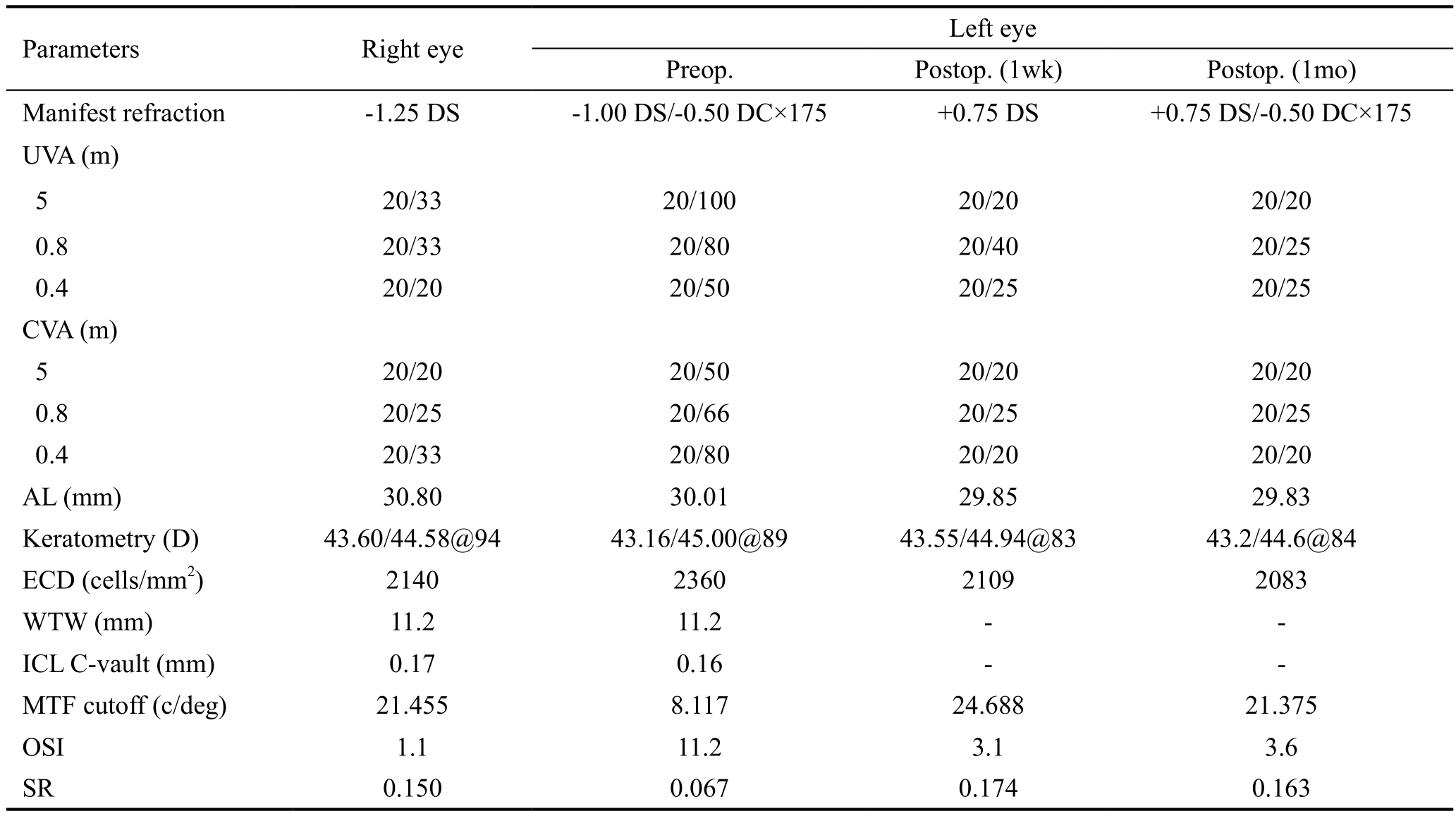
UVA: Uncorrected visual acuity; CVA: Corrected visual acuity; AL: Axial length; ECD: Endothelial cell density; ICL: Implantable collamer lens; C-vault: Central vault; MTF: Modulation transfer function; OSI: Objective scattering index; SR: Strehl ratio.
In most cases, we chose monofocal IOL for patients with cataract and extra-high myopia, rather than trifocal IOL,because of the retinal complications or possibly increasing AL.In this case, the patient was a 44-year-old teacher, requiring high visual quality in intermediate and near distance while working, and the importance of far vision could not be ignored for daily life at the same time. After evaluating the AL and retina, we found that the situation of this patient was relatively stable (AL: OD 30.63 mm, OS 29.86 mm in 2014 before ICL implantation, OD 30.80 mm OS 30.01 mm in 2016 with ICL;without obvious vision-threatened retinal disorders). Besides,the patient’s own crystalline lens reserved the accommondation in the right eye. A diffractive trifocal IOL implantation in the left eye would be helpful to maintain the balance of vision at far, intermediate, near distance, and brought better binocular visual function, thus enhanced the patient’s life quality. A 6-year follow-up showed multifocal IOL implantation in the high myopia provided optimal binocular visual comfort, only 2 rhegmatogenous retinal detachments (3.8%) and one case of macular atrophy, 98% patients reached best CVA of at least 0.5 and 38% of at least 0.8 without correction[14]. From here we saw that high myopia was not an absolute contraindication of multifocal IOL implantation.
In the current case, the patient with a working-age of 44-year-old underwent the ICL explantation, standard phacoemulsification and AT LISA tri 839MP implantation monocularly. The trifocal IOL provided excellent results in visual acuity at far, intermediate and near distance; high patient satisfaction with spectacle independence and no obvious optical disruption during the follow up. However, residual hyperopia of the left eye was +0.5 D SE at 1mo regretfully postoperatively. As it was reported, a longer postoperative AL after ICL implantation with a mean difference of 0.054 mm by IOL-Master[15]. We attributed the postoperative residual hyperopia to the inaccurate preoperative AL measuring by IOL-Master, which might result in a slight disturbance in calculating the IOL power. We remeasured the postoperative AL of the left eye at 1mo, and found the AL turned to be 29.83 mm, 0.18 mm shorter than preoperative AL (30.01 mm).Taking in account the above, we supposed that it is necessary to consider the preoperative AL measurement of ICL patient for cataract surgery, especially for accurate trifocal IOL implantation.
In summary, our case indicates the use of a diffractive trifocal IOL (AT LISA tri 839MP) to be beneficial for the treatment of clinically symptomatic cataract monoculary induced by a low ICL vault in patient at a working-age. Concerns for accurate high-end IOL power calculation in eyes with phakic IOL in situ should be studied in the future.
Foundation:Supported partly by the General Natural Science Projects, Department of Education, Zhejiang Province, China(No.Y201636718).
Conflicts of Interest: Chen SY,None;Xie C,None;Wang Y,None;Shen Y,None.
REFERENCES
1 Lee J, Kim Y, Park S, Bae J, Lee S, Park Y, Lee J, Lee JE. Long-term clinical results of posterior chamber phakic intraocular lens implantation to correct myopia.Clin Exp Ophthalmol2016;44(6):481-487.
2 Guber I, Mouvet V, Bergin C, Perritaz S, Othenin-Girard P, Majo F.Clinical outcomes and cataract formation rates in eyes 10 years after posterior phakic lens implantation for myopia.JAMA Ophthalmol2016.[Epub ahead of print]
3 Sanders D, Vukich JA. Comparison of implantable collamer lens (ICL)and laser-assisted in situ keratomileusis (LASIK) for low myopia.Cornea2006;5(10):1139-1146.
4 Sanders DR, Doney K, Poco M; ICL in Treatment of Myopia Study Group. United States Food and Drug Administration clinical trial of the implantable collamer lens (ICL) for moderate to high myopia: three-year follow-up.Ophthalmology2004;111(9):1683-1692.
5 Cao X, Wu W, Wang Y, Xie C, Shen Y. Comparison over time of vault in chinese eyes receiving implantable contact lenses with or without a central hole.Am J Ophthalmol2016;172:111-117.
6 Cao X, Tong J, Wang Y, Zhou T, Ye B, Li X, Shen Y. Long-term ultrasound biomicroscopy observation of position changes of a copolymer posterior chamber phakic intraocular lens.J Cataract Refract Surg2014;40(9):1454-1461.
7 Cochener B, Vryghem J, Rozot P, Lesieur G, Chevalier JP, Henry JM,David T, Lesueur L, Gatinel D, Ganem C, Blanckaert J, Van Acker E,Heireman S, Ghekiere S. Clinical outcomes with a trifocal intraocular lens: a multicenter study.J Refract Surg2014;30(11):762-768.
8 Chen C, Xu X, Miao Y, Zheng G, Sun Y, Xu X. Accuracy of intraocular lens power formulas involving 148 eyes with long axial lengths: a retrospective chart-review study.J Ophthalmol2015;2015:976847.
9 Bang S, Edell E, Yu Q, Pratzer K, Stark W. Accuracy of intraocular lens calculations using the IOLMaster in eyes with long axial length and a comparison of various formulas.Ophthalmology2011;118(3):503-506.
10 Eom Y, Song JS, Kim HM. Spectacle plane add power of multifocal intraocular lenses according to effective lens position.Can J Ophthalmol2017;52(1):54-60.
11 Maeng HS, Chung TY, Lee DH, Chung ES. Risk factor evaluation for cataract development in patients with low vaulting after phakic intraocular lens implantation.J Cataract Refract Surg2011;37(5):881-885.
12 Kohnen T, Titke C, Bohm M. Trifocal intraocular lens implantation to treat visual demands in various distances following lens removal.Am J Ophthalmol2016;161:71-77.e1.
13 Mojzis P, Majerova K, Plaza-Puche AB, Hrckova L, Alio JL. Visual outcomes of a new toric trifocal diffractive intraocular lens.J Cataract Refract Surg2015;41(12):2695-2706.
14 Martiano D, Cochener B. Multifocal IOLs in the high myope, 6-year follow-up.J Fr Ophtalmol2014;37(5):393-399.
15 Yu A, Wang Q, Zhu S, Xue A, Su Y, Pan R. Effects of posterior chamber phakic intraocular lens on axial length measurements.Zhonghua Yan Ke Za Zhi2015;51(3):206-209.
Correspondence to:Ye Shen. Department of Ophthalmology,the First Affiliated Hospital, College of Medicine, Zhejiang University, 79 Qingchun Road, Hangzhou 310003, Zhejiang Province, China. idrshen@zju.edu.cn
Received:2017-12-09 Accepted: 2018-03-12
DOl:10.18240/ijo.2018.07.27
Citation:Chen SY, Xie C, Wang Y, Shen Y. Full-vision maintenance in extra-high myopia from implantable collamer lens to trifocal intraocular lens implantation. Int J Ophthalmol 2018;11(7):1239-1242