Comparison of diathermic high-frequency capsulorhexis and continuous curvilinear capsulorrhexis in white cataract surgery
Li Wang1,2, Peng Li3, Xiong Guo2
1Department of Ophthalmology, Department of Medical and Research Technology Xi’an Medical University, Xi’an 710021,Shaanxi Province, China
2School of Public Health, Health Science Center, Xi’an Jiaotong University, Xi’an 710061, Shaanxi Province, China
3Department of Ophthalmology, the 451stHospital of the PLA,Xi’an 710054, Shaanxi Province, China
INTRODUCTION
The history of cataract surgery is a continuous improvement in the surgical concept and technology from intracapsular cataract extraction, extracapsular cataract extraction to the present phacoemulsification (PHACO). The most critical step and one of the most elusive techniques in cataract surgery is successful anterior capsulotomy[1]. At present, continuous curvilinear capsulorrhexis (CCC) is the most commonly used technique in clinic. It makes use of discission needle or capsulotomic forcep to perform mechanical blunt separation.During this separation, firstly, identify the local opening, force tension artificially follow a circular trace and tear the anterior capsule. The end of the track merges with the initial opening to tear the anterior lens capsule. CCC is an important step in PHACO combined with intraocular lens (IOL) implantation[2].
The quality of the capsulorhexis directly determines the safety of subsequent operations and stability of IOL[3]. However,for white mature cataracts, surgeons fail to clearly identify anterior lens capsule and the tearing opening because of poor red fundus reflex and the larger capsule tension, which makes it more difficult to perform the capsulorhexis. It is reported that CCC used for patients with white mature cataract has high failure rate[4]. In recent years, diathermic high-frequency capsulorhexis (DHC) has been applied in white cataract, which is mainly conducting high frequency power to discission needle tip covered on the handle by taking advantage of electrocoagulation main engine. Heating effect brought by discission needle would help to complete the posterior CCC[5-6].
This study mainly focuses on the ultrastructure differences of anterior lens capsule derived from the above two surgical methods under optical microscopy and transmission electron microscopy (TEM) respectively, and records the completion conditions of CCC and corneal endothelial cell counts preand post-operation in both groups. To investigate that whether DHC would cause damage to lens epithelial cells and furthurly study that whether the damage has the impact on the stability of capsule, thus to guide the selection of capsulorhexis methods for surgeons.
SUBJUCTS AND METHODS
SubjectsSubjects were recruited from the 451stHospital of the PLA from June 2014 to November 2016. A total of 66 patients (66 eyes) aged between 60 and 80y (mean 72.5±5.5) did the surgery (33 males and 33 females). They were randomly divided into two groups according to random number table: group A (DHC, 33 patients) and group B (CCC,33 patiens). Sixteen cases from group A were observed by TEM and 17 cases were observed by optical microscopy through random number table. So did the group B. The operation was performed under the topical anaesthesia of 0.5%oxybuprocaine. As described in the previous literatures, the group B performed the CCC with capsulorhexis forceps,6 mm in diameter. Group A adopted diathermic capsulorhexis needle in Catarhex PHACO instrument (Oertli, Switzerland).The needle entered into the anterior chamber after the injection of viscoelastic solution (the current intensity accounts for 70%-80% of the total intensity output from the instrument).The electrode of the capsulorhexis needle tip gently pressed the anterior capsule to move slowly at a constant speed, anticlockwise following the circular track to complete the CCC with 5.5-6.0 mm in diameter. A round of vacuoles flushed on the anterior capsule. All the PHACO were successfully completed by the same surgeon (Li P). The study was approved by local Institutional Enthnic Committee of the 451stHospital of the PLA and met the tenets of the Declaration of Helsinki.The informed consent was obtained from the participants.
Optical Microscopy ExaminationThe anterior lens capsule was removed and placed on smooth and clean glass slide immediately. Spread it out and put on the slide with a forceps under optical microscopy, after ethanol dehydration and HE-staining, observe it under the OlympusBX51 optical microscopy.
Transmission Electron Microscopy ExaminationThis experiment was implemented in Electron Microscopy Center,Xi’an Jiaotong University Health Science Center. The anterior lens capsules were derived and placed into 2.5% precooled glutaraldehyde stationary liquid (0.1 mol/L phosphate buffer and 4% paraformaldehyde) over 2h at 4℃, embathed in 0.1 mol/L phosphate buffer for 30min, fixed with 1% osmium tetroxide stationary liquid (0.1 mol/L phosphate buffer) at 4℃ for 2h,washed with 0.1 mol/L phosphate buffer for 10min. Ethanol gradient dehydration: 30% ethanol for 10min, 50% ethanol for 10min and 70% ethanol for 10min. Stained with 70%uranyl acetate for 2h and stayed overnight. And then replaced and stayed with propylene epoxide for 10min. Soaked,embedded and polymerized with Epoxy resin Epon812 and cutted into semi-ultrathin sections for 1-2 µm. Located under the optical microscope after methylene blue staining. LKB-V ultramicrotome (Sweden) was used to perform the ultrathin section for 50-70 nm. The slices were observed and taken photos under the TEM (H-600, H-7650 and JEM-100SX;Hitachi, Ltd. Japan) after stained with uranyl acetate and lead citrate. The surgical completion and corneal endothelial cell counts of the two groups pre- and post-operation were recorded.
Statistical MethodsSPSS17.0 statistical software was used for data processing. Chi-square test was adopted in groupcomparison. Corneal endothelial cell counts between two groups was compared with t-test. The paired t-test was used to compare the eyesight and corneal endothelial cell counts within each group pre- and post-operation. A P value of ˂0.05 was considered statistically significant difference.
RESULTS
Anterior Lens Capsule Derived from Continuous Curvilinear Capsulorrhexis
Optical microscopyOptical microscopy showed intact cell nucleus within anterior lens capsule with well-organized cells,distinct boundaries among cells and intact cell structure at the edge of anterior lens capsule (Figure 1A).
Transmission electron microscopyTEM showed the mean thickness of anterior capsule of all samples were 22 µm.The cells of anterior lens capsule lined up neatly and closely connected with the basement membrane. The free surface of the cells were smooth and flat (Figure 1C, 1D). The organelles in cytoplasm were abundant and the mitochondrias were slight swelling. Endoplasmic reticulum in the form of short rod were scattered around nucleus and finger-like interdigitation could be seen in intercellular (Figure 1E).
Anterior Lens Capsule Derived from Diathermic Highfrequency Capsulorhexis
Optical microscopyOptical microscopy showed an acellular necrotic area with unequal width at the edge of anterior lens capsule, which had been estimated as thermal damage area.The cell free area presented light pink after HE-staining. The edge of the anterior capsule showed uneven with a larger odontoid and irregular bump compared with that of CCC(Figure 1B).
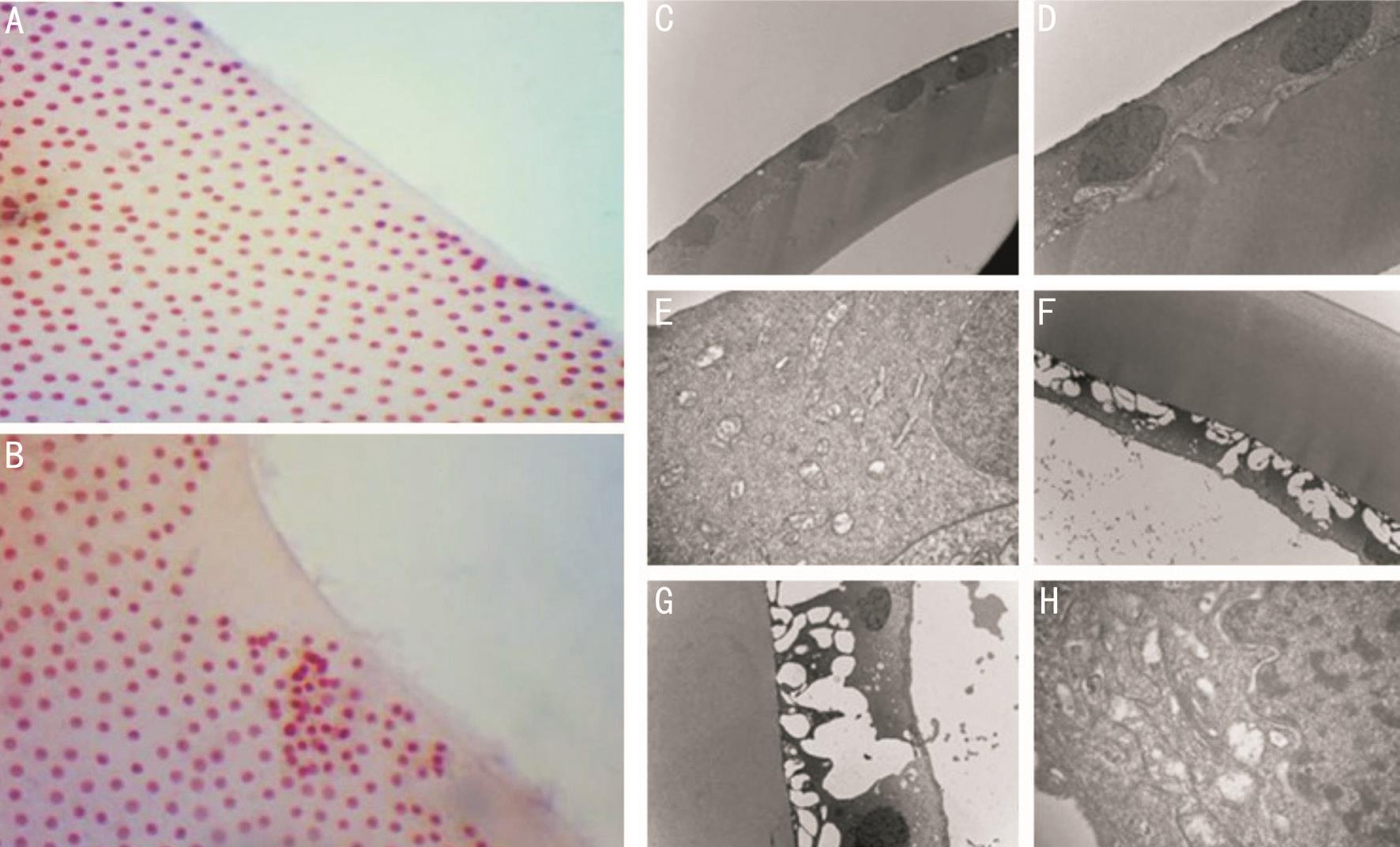
Figure 1 Anterior lens capsule A: Derived from CCC observed by Olympus BX 51 optical microscopy (images magnification ×40); B:Derived from DHC observed by Olympus BX 51 optical microscopy (images magnification ×40); C: Derived from CCC observed by TEM(images magnification ×2500); D: Derived from CCC observed by TEM (images magnification ×6000); E: Derived from CCC observed by TEM(images magnification ×30 000); F: Derived from DHC observed by TEM (images magnification ×2500); G: Derived from DHC observed by TEM (images magnification ×6000); H: Derived from DHC observed by TEM (images magnification ×50 000).
Table 1 Comparison of two kinds of capsulorhexis n (%)

CCC: Continuous curvilinear capsulorrhexis; DHC: Diathermic high-frequency capsulorhexis.
Groups Cases Corneal endothelial cell density (mm2)Total Successful Implanted capsular bag Preop. 1wk postop.CCC 33 24 (72.7) 28 (84.8) 2232.55±185.28 2025.36±165.42 DHC 33 31 (93.9) 33 (100.0) 2246.21±184.62 2012.87±170.26
Transmission electron microscopy examinationTEM showed shrinkage of lens epithelial cells 11 µm distance from the edge of the anterior lens capsule and cell nucleus could be seen at the 40 µm from the edge of the anterior lens capsule(Figure 1F). There were many odontoid processes and foveae connected continually at the edge of anterior lens capsule(Figure 1G). Anterior lens capsule cells were monolayer cube-like epithelial cell, part of which showed swelling.Electron density was reduced. The connection of cells and basement membranes were loosened. The cell free surface was unsmooth. The organelles in cytoplasm were abundant and the mitochondrias were slight swelling. Endoplasmic reticulum was slight expanded. The intercellular connection was loosened. What of the above made the cells had a netlike appearance (Figure 1H).
Corneal Endothelial Cell CountsThe anterior corneal endothelial cell densities between group A and group B preoperation showed no statistical difference (t=1.22, P˃0.05).The counts declines in both groups 1wk post-operation (t=3.52,4.03, P˂0.05 in both). However, there was no statistical difference between the two groups (t=1.63, P˃0.05; Table 1).
Comparison of Capsulorhexis Conditions Between Two GroupsNine cases of group A suffered from anterior capsule rupture during operation because the capsular bag split up to the periphery by itself; 5 cases of which suffered from posterior capsule rupture, the IOL was implanted into the ciliary groove.The success rate of group A was 72.7%. Two cases of group B suffered from anterior capsule rupture due to the high pressure when piercing the anterior capsule. Diathermic capsulorhexis supplement in time could stop the gap backward outspread,which avoided the posterior capsular rupture. IOLs were successfully implanted into the capsular bags. The success rate of group B reached to 93.9%, which was apparently higher than that of group A (χ2=2.452, P=0.023).
DISCUSSION
Cataract, at present, is the most common blinding eye disease which can be treated with surgery. Nowadays, PHACO combined with IOL implantation is mature. The results of capsulorhexis have directly impact on the follow-up procedures of cataract surgery. Theoretically, intact capsular bag opening is the important guarantee of crushing and chopping of cataract nucleus, and sucking out of cortex. More than 20y ago, CCC was invented by Gimbel and Neuhann[7], which has been the key of PHACO. It has the advantage that the edge of anterior capsular bag opening has high tenacity without fracture, which makes it able to withstand large external forces. Anterior lens capsule composed of human collagen type IV, is a layer of uniform-in-texture and elastic tissue membrane without collagenous fiber, so that there is no directionality when operating the capsulorhexis. With the influence of people education degree, knowledge of diseases and economic level etc., a great many patients with white mature or hypermature cataract can be met in clinic in some developing countries and regions. Degeneration, calcification, macular densa, and other hard lens nucleus (grade IV/V) often occur in anterior lens capsules of patients in these areas. Some of them have cortex liquefaction, increased brittleness, decreased red reflex in fundus and cortex liquefaction leakage. which bring many difficulties for the operation. What’s more, CCC of both liquefied and non-liquefied white cataract will be challenges for physicians. Operations for these kinds of cataracts are always characterized by a shallow anterior chamber with small operating space and unclear capsule. Even though the liquefied cortex is sucked out, the application of CCC and the track are still hard to control, thus affect the smooth capsulorhexis.Furthermore, the broken of intumescent lens cortex will destroy the foundation bed appressed with lens capsule. It’s hard to control the tearing track of ultrathin capsule due to intumescent lens, tensed capsule and unbalanced capsule tension. Sometimes, the surgeons even cannot get a tearing chance, which will lead to a serious deviation from the track or a radial capsulorhexis[8-10]. Recently, there are several staining agents, such as trypan blue, fluorescein, gentian violet,indocyanine green and so on, having been used for capsule staining. However, there is only trypan blue approved by the FDA. Studies proposed that trypan blue can harden the anterior capsule, which increase the possibility of rupture of anterior capsule, as well as the residual, corneal toxicity and irritability by staining agents like trypan blue and indocyanine green[11]. Clinically, although the stain are helpful to distinguish capsulorhexis of white cataract, it fails to improve capsule tension, so that the operation is still not easy and it is hard to universally be used in primary hospital due to the rare material.Plenty of clinical experience and highly adept operative skills are necessary for a perfect cataract capsulorhexis. Therefore,looking for a good capsulorhexis technique has been a goal in ophthalmologists[12]. The application of annular DHC is a relatively safe technique with the results same to the CCC.There is high frequency energy from electrocoagulation main engine on the discission needle tip covered on the handle.Heating effect brought by discission needle would help to complete the CCC. The learning curve of this operation is short, easy to master and with good and optional domination,especially when the conventional capsulorhexis fails to control the track, diathermic capsulorhexis will be the replacement at once to guarantee the operation results.
In this study, anterior lens capsule derived from DHC when observed under optical microscopy is rounder than that of CCC in shape, but the edge is not very smooth. While observed under TEM, the edge of anterior lens capsule derived from DHC is an cell free area, with distinct arc-shaped and homogeneous tissue. Part of the edge is much less smooth. There is a 60 µm denatured necrotic zone at the edge of anterior lens capsule derived from diathermic capsulorhexis. The interior lens epithelial cells are incomplete, the ultrastructure is damaged by diathermic capsulorhexis and the edge is rougher when compared with that of CCC. There is no denatured necrotic zone at the edge of anterior lens capsule taken down by CCC.This result is connected with the heating effect of DHC.The continuous heating effect links burning points to lines,lines to surfaces for the final tissue cutting. Lens epithelial cells of anterior lens capsule taken down by high-frequency capsulorhexis is observed as slight retraction, crimping and thickening under TEM. Stained cell nucleus is visible 40-60 µm from the edge. The cell free area should be related to the effect of DHC. The anterior capsule opening made by DHC is tough and safe. That’s because the effect of diathermic high-frequency has enlarged and strengthened the anti-tensile strength and elastic pulling force of the circular and incrassated edge, which makes the lens nucleus fulfill phacofragmentation in situ in capsular bag. IOL can be steadily implanted into capsular bag to avoid epithelial cell remaining which will leads to the fiber persistent contraction caused by capsule opacification, fibrocyte formation and metaplasia, as well as IOL displacement or other complications. The comparison of corneal endothelial cell counts results between two methods is not particularly different, which indicates that the heating effect of DHC has no obvious damage on corneal endothelium.In recent years, in the capsulorhexis technique of cataract surgery, femtosecond laser is also used in the capsulorhexis of white cataract and is an ideal capsulorhexis technique.Theoretically, the edge of CCC by femtosecond laser is smooth with a middle location and the laser can design a capsule opening randomly, with which the other CCC technique is not good enough to compare[13-18]. However, femtosecond laser is hard in popularization and promotion due to the economic reasons. Meanwhile, capsular block syndrome and a high incidence of early stage posterior capsular opcaification after operation are easy to occur when use femtosecond laser to perform CCC[19]. With the characteristics of simpleness and convenience, the DHC is a helpful capsulorhexis due to its special practicability in the popularization circumstance of PHACO. Although the operation time is longer than other methods, DHC can ensure that the operation goes smoothly.Therefore, DHC has good clinical application value in white mature and hypermature cataract surgery[20]. From another point of view, this study provides clinical and ultrastructure evidence on how to select capsulorhexis and the stability of capsule opening for white cataract surgery.
ACKNOWLEDGEMENTS
The authors wound like to thank Guo X for precious guidance.
Foundation:Supported by the Shaanxi Provincial Department of Science and Technology Agency Project (No.2017SF-288).
Conflicts of Interest:Wang L, None; Li P, None; Guo X,None.
REFERENCES
1 Srinivasan S. Capsulorhexis: the perfect circle. J Cataract Refract Surg 2017;43(3):303-304.
2 Zeng Y, Gao JH. Continuous curvilinear capsulorhexis in cataract surgery using a modified 3-bend cystotome. J Ophthalmol 2015;2015:412810.
3 Findl O, Hirnschall N, Draschl P, Wiesinger J. Effect of manual capsulorhexis size and position on intraocular lens tilt, centration, and axial position. J Cataract Refract Surg 2017;43(7):902-908.
4 Kucukevcilioglu M, Koylu MT, Mutlu FM. A novel capsulorhexis technique in white cataract surgery. Semin Ophthalmol 2017;32(5):661.
5 Wang WH, Wu XY, Zhang JL. Application of highfrequency electrical capsulotomy in maturation period cataractsurgery. Guoji Yanke Zazhi (Int Eye Sci) 2016;16(10):1927-1928.
6 Yuan JM, Wang H, Tan XF, Quan CJ, Nie X, Yang XH. The application of high frequency electrical capsulotomy instruments in phacoemulsification of hypermaturecataract. J Clinical Ophthalmol 2014;22(3): 211-213.
7 Gimbel HV, Neuhann T. Development, advantages, and methods of the continuous circular capsulorhexis technique. J Cataract Refract Surg 1990;16(1):31-37.
8 Chee SP, Chan NS. Capsule milking: modification of capsulorhexis technique for intumescent cataract. J Cataract Refract Surg 2017;43(54):585-589.
9 Moshirfar M, Skanchy DF, Shah T. Intraoperative management of anterior capsular tear. Curr Opin Ophthalmol 2017;28(1):42-48.
10 Nabil KM. Lens decompression technique for prevention of intraoperative complications during phacoemulsification of intumescent cataract. Indian J Ophthalmol 2017;65(12):1436-1439.
11 Lotfy A, Abdelrahman A. Trypan blue-assisted posterior capsulorhexis in pediatric cataract surgery. Clin Ophthalmol 2017;11:219-222.
12 Soylak M. Novel device for creating continuous curvilinear capsulorhexis. Springerplus 2016;5(1):2053.
13 Takagi M, Kojima T, Ichikawa K, Tanaka Y, Kato Y, Horai R, Tamaoki A, Ichikawa K. Comparison of maximum stretch forces between femtosecond laser-assisted capsulotomy and continuous curvilinear capsulorhexis. J Ophthalmol 2017;2017:3489373.
14 Qian DW, Guo HK, Jin SL, Zhang HY, Li YC. Femtosecond laser capsulotomy versus manual capsulotomy: a Meta-analysis. Int J Ophthalmol 2016;9(3):453-458.
15 Dick HB, Schultz T. A review of laser-assisted versus traditional hacoemulsification cataract surgery. Ophthalmol Ther 2017;6(1):7-18.
16 Kanellopoulos AJ, Asimellis G. Standard manual capsulorhexis/ultrasound phacoemulsification compared to femtosecond laser-assisted capsulorhexis and lens fragmentation in clear cornea small incision cataract surgery. Eye Vis (Lond) 2016;3:20.
17 Christy JS, Nath M, Mouttapa F, Venkatesh R. Learning curve of femtosecond laser-assisted cataract surgery: experience of surgeons new to femtosecond laser platform. Indian J Ophthalmol 2017;65(8):683-689.
18 Chan T, Pattamatta U, Butlin M, Meades K, Bala C. Intereye comparison of femtosecond laser-assisted cataract surgery capsulotomy and manual capsulorhexis edge strength. J Cataract Refract Surg 2017;43(4):480-485.
19 Rostami B, Tian J, Jackson N, Karanjia R, Lu K. High rate of early posterior capsule opacification following femtosecond laser-assisted cataract surgery. Case Rep Ophthalmol 2016;7(3):213-217.
20 Weng CH, Wu LC, Xu TT, Xu D, Zhou XT. Application of electrical capsulotomy tip in phacoemulsification for white cataract. Recent Advance in Ophthalmology 2016;36(5):450-452.
Correspondenceto:Li Wang. Department of Ophthalmology,Department of Medical and Research Technology Xi’an Medical University, Xi’an 710021, Shaanxi Province, China.teawangli@126.com
Received:2017-03-14 Accepted: 2018-05-30
Abstract● AlM: To compare the corneal endothelial cell counts pre- and post-operation, ultrastructure of anterior lens capsule and surgical completion after diathermic highfrequency capsulorhexis (DHC) and continuous curvilinear capsulorrhexis (CCC) applied in phacoemulsification(PHACO) of white cataract surgery.● METHODS: Sixty-six eyes of 66 patients (33 males and 33 females) with cataract aged between 60 and 80y (mean 72.5±5.5) were recruited and undergone the surgery from June 2014 to November 2016. Anterior lens capsule,derived from two kinds of capsulorhexis, were randomly divided into two groups according to random number table. The ultrastructure of the capsule edge and its closer tissue were observed by transmission electron microscopy(TEM) and optical microscopy respectively. The surgical completion conditions and corneal endothelial cell counts were analyzed pre- and post-operation after two capsulorhexis.● RESULTS: The capsule derived from CCC had smooth edge, well-organized cellular structure and the cells filling into the cutting edge under TEM and optical microscopy.The capsule derived from DHC had an approximate 60 banded area of cell degeneration and necrosis, with dentiform prominences at the edge of the capsule, and no cell structure was observed at this area. The corneal endothelial cell counts of both groups were slightly declined 1wk post-operation compared with that of preoperation. There was no statistical difference between the two groups (t=1.63, P>0.05).● CONCLUSlON: DHC shows good clinical value in white mature and hypermature cataract surgery.
● KEYWORDS:diathermic high-frequency capsulorhexis;continuous curvilinear capsulorrhexis; ultrastructure; corneal endothelial cell
DOl:10.18240/ijo.2018.08.11
Citation:Wang L, Li P, Guo X. Comparison of diathermic highfrequency capsulorhexis and continuous curvilinear capsulorrhexis in white cataract surgery. Int J Ophthalmol 2018;11(8):1317-1321