lnvestigation of possible risk factors in the development of seasonal allergic conjunctivitis
Ümit Doğan 1 , Sümeyra Ağca 2
1 Department of Ophthalmology, Medical Faculty, Abant Izzet Baysal University, Bolu 14280, Turkey
2 Department of Ophthalmology, Ardahan State Hospital,Ardahan 75000, Turkey
Abstract · AlM: To analyze the possible risk factors in the development of seasonal allergic conjunctivitis (SAC)through an evaluation of skin allergy tests and data obtained from questionnaires.· METHODS: The study included a total of 75 SAC patients and 71 control subjects without SAC diagnosis who were admitted to the Abant lzzet Baysal University Medical Faculty Ophthalmology Clinic between March 2016 and December 2016. Skin prick tests were performed for all participants. Serum levels of total lgE and 25-OH vitamin D were also measured. ln the tear, total lgE levels were measured. Moreover, possible risk factors for the onset of SAC (smoking, paracetamol exposure, vitamin D supplementation and environmental factors etc. ) were examined for all patients by both prenatal and postnatal aspects.· RESULTS: The patients with SAC were found to have a history of maternal paracetamol exposure during the prenatal period. Likewise, in the same patient group, the duration of postnatal vitamin D supplementation was shorter ( P <0.001). However, no significant correlation was found between SAC and maternal antibiotic exposure,maternal smoking, the mode of delivery and birth weight,as well as presence of pets. Moreover, patients with SAC were more likely to have asthma, allergic rhinitis and oral allergy syndrome. We have also found that SAC patients’mothers and siblings were more likely to have allergic conjunctivitis. Likewise, their fathers were more likely to have allergic rhinitis.· CONCLUSlON: Prenatal maternal paracetamol exposure and shorter duration of vitamin D supplementation in the postnatal period may play a role in development of SAC. Therefore prevention of unnecessary gestational paracetamol intake and vitamin D supplementation during infancy could potentially reduce the onset and development of SAC.
· KEYWORDS: conjunctival disease; seasonal allergic conjunctivitis; type I hypersensitivity reaction
INTRODUCTION
Seasonal allergic conjunctivitis (SAC) is a disease, which affect the ocular surface via type I hypersensitivity reaction, with an incidence rate of 5% to 22% [1-3] . Ocular allergic inflammation is a very common event due to frequent contact of the eye with environmental allergens. It is known that serum and tear eosinophil counts and immunoglobulin E(IgE) levels may be high because of the type I hypersensitivity reaction in the etiology of this disease [3-6] . A good review of available epidemiological data about SAC prevalence can reassure the physician at diagnosis and allow early initiation of treatment [6] . The possibility of diagnosis and treatment of SAC can be improved with studies examining the life quality and lifestyles of SAC patients as well as calculating the SAC prevalence [6] . The incidence of SAC has been found to be high in patients with allergic asthma and allergic rhinitis.Moreover, the role of vitamin D, which is an immune system activator and has frequently been used in cancer treatment in recent years, remains controversial in reducing the incidence of SAC [7-10] . The aim of this study was to develop proposals for the identification of predisposing factors of SAC. Therefore,an evaluation was performed in SAC patients regarding perinatal risk factors, familial allergy history, dietary patterns,owing pets, age at first contact with pets, and vitamin D supplementation during infancy.
SUBJECTS AND METHODS
The study was performed in adherence with the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Abant Izzet Baysal University Medical Faculty(Number: 2016/15). The SAC group included 75 patients (30 females and 45 males) with SAC aged between 7 to 30 years old, who were admitted to the Abant Izzet Baysal UniversityMedical Faculty Ophthalmology Clinic between March 2016 and December 2016. The control group (CG) was comprised of 71 patients (29 females and 42 males) aged between 8 to 29 years old (Table 1). Patients with active ocular infection or severe ocular pathology, xerophthalmia history, and blepharitis,those who had undergone eye surgery in the previous 3mo,contact lens users, and females who were pregnant or nursing mothers were excluded from the study. A written informed consent was obtained from all patients or from the parents of patients, who were under the age of 18.
Table 1 Demographic, hemogram, serum-tear IgE, serum vitamin D, atopy presence and allergic conjunctivitis scoring data of the allergic conjunctivitis and CG
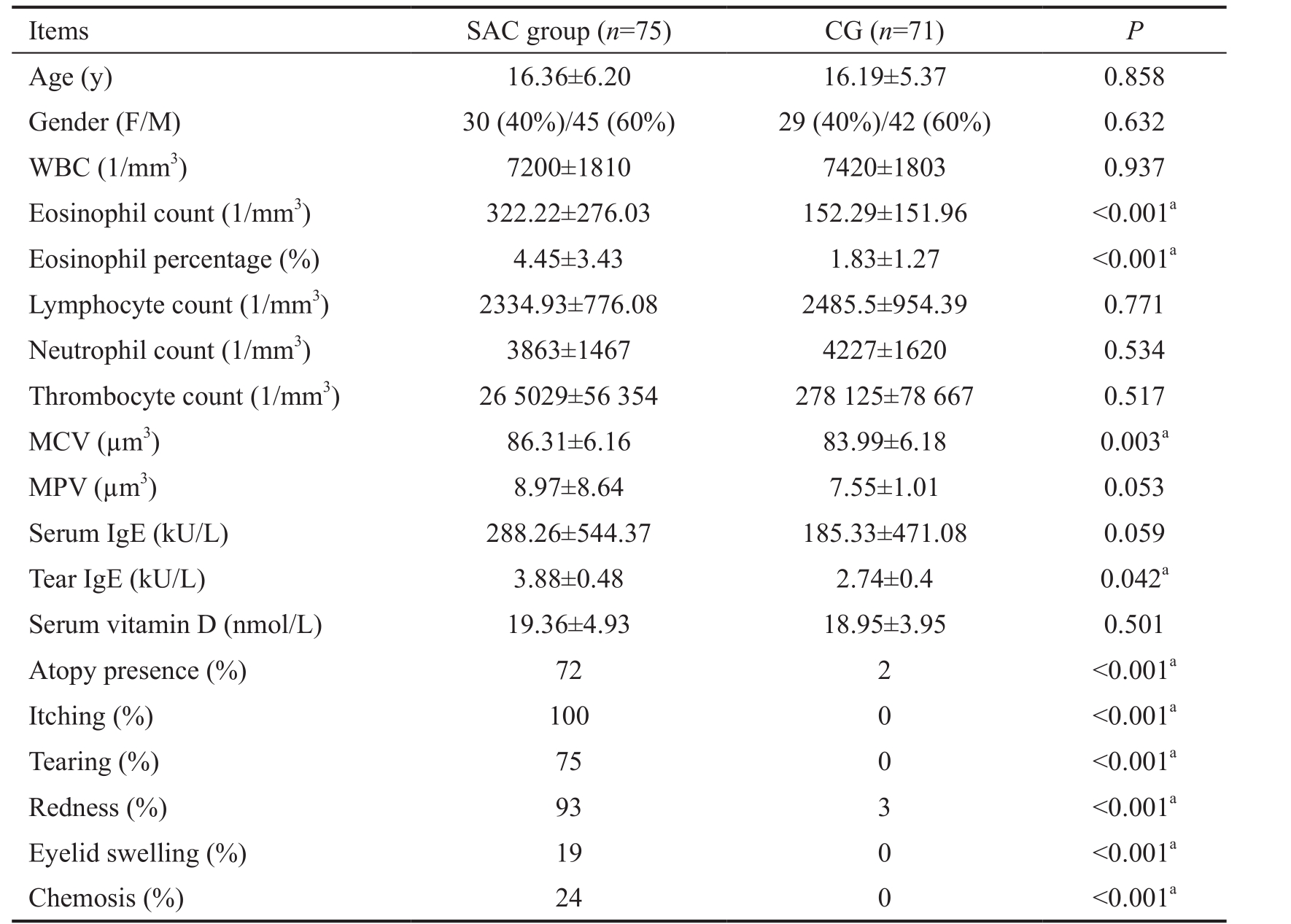
SAC: Seasonal allergic conjunctivitis; CG: Control group; WBC: Leukocyte count; MCV: Mean erythrocyte volume; MPV: Mean thrombocyte volume. a P <0.05 was accepted as statistically significant.
Items SAC group ( n =75) CG ( n =71) P Age (y) 16.36±6.20 16.19±5.37 0.858 Gender (F/M) 30 (40%)/45 (60%) 29 (40%)/42 (60%) 0.632 WBC (1/mm 3 ) 7200±1810 7420±1803 0.937 Eosinophil count (1/mm 3 ) 322.22±276.03 152.29±151.96 <0.001 a Eosinophil percentage (%) 4.45±3.43 1.83±1.27 <0.001 a Lymphocyte count (1/mm 3 ) 2334.93±776.08 2485.5±954.39 0.771 Neutrophil count (1/mm 3 ) 3863±1467 4227±1620 0.534 Thrombocyte count (1/mm 3 ) 26 5029±56 354 278 125±78 667 0.517 MCV (µm 3 ) 86.31±6.16 83.99±6.18 0.003 a MPV (µm 3 ) 8.97±8.64 7.55±1.01 0.053 Serum IgE (kU/L) 288.26±544.37 185.33±471.08 0.059 Tear IgE (kU/L) 3.88±0.48 2.74±0.4 0.042 a Serum vitamin D (nmol/L) 19.36±4.93 18.95±3.95 0.501 Atopy presence (%) 72 2 <0.001 a Itching (%) 100 0 <0.001 a Tearing (%) 75 0 <0.001 a Redness (%) 93 3 <0.001 a Eyelid swelling (%) 19 0 <0.001 a Chemosis (%) 24 0 <0.001 a
All participants underwent detailed physical and ophthalmologic examinations. The diagnosis of SAC was made from evaluation of the complaints and the findings of itching,tearing, redness, chemosis and eyelid edema. Itching was evaluated by the subjects using a standardized scale (0=no itching; 4=severe itching). Redness, eyelid swelling, chemosis and tearing were evaluated by the researchers using the standardized scales (0=none; 3=severe) [11] . During individual face-to-face interviews conducted using a questionnaire,detailed background and family information were collected in terms of possible risk factors for the development of allergic conjunctivitis. In all subjects, total IgE levels in the tear, serum levels of total IgE and serum levels of 25-OH vitamin D were measured. The skin prick test was applied to determine the sensitivity to any allergen.
Biochemical Analysis Tears of the patients were collected into the 75 μL hematocrit tubes (Haemotocrit-Kapillaren,Hirschmann Laborgerate, Germany). The hematocrit tubes were placed in the lateral cantus to collect from the inferior tear meniscus. The samples were stored at -80℃ in air proof microcentrifuge tubes.
The blood samples were centrifuged at 2000 rpm for 15min to separate serum and plasma. All tubes were labeled and stored at -80℃ until analysis. The serum and plasma samples were then thawed and brought to room temperature for analysis. The plasma 25-OH vitamin D and serum IgE levels were tested using the electrochemiluminescence method using an Elecsys 2010 analyzer (Roche Diagnostics, Mannheim, Germany). The detection limit for 25-OH vitamin D was 3 ng/mL (7.5 nmol/L).The detection limit for IgE was 0.10 IU/mL (0.24 ng/mL). The tear IgE level was tested using the same methods. All samples were coded and studied as a single blinded method.
Skin Prick Tests Skin prick tests were applied to all participants to determine atopy in the presence of respiratory allergens [house dust mites (D pteronyssinus, D farinae), cats, dogs, cockroach,fungi (Alternaria, Aspergillus, Clodosporium) and pollen mixtures (weeds, cereals, grasses and trees]. The skin prick tests were evaluated 15-20min after the epidermal application of positive control, negative control, and allergens to the forearm. Values with an induration diameter of 3 mm greater than the negative value were accepted as positive for atopy.
Statistical Analysis For the statistical analysis, the Student- t test and Mann-Whitney U test were used to compare the groups and the Spearman correlation test was used for the correlation analysis. All categorical variables were compared between the groups using Chi-square test. SPSS 22 (IBM SPSS Statistics; IBM, Armonk, NY, USA) were used to perform statistical analyses.
RESULTS
The study included a total of 75 patients with SAC and 71 control subjects. The SAC group consisted of 30 (40%)females and 45 (60%) males with a mean age of 16.36±6.2y.The CG consisted of 29 (40%) females and 42 (60%) males with a mean age of 16.19±5.37y. The age and gender were statistically similar between the two groups ( P =0.858; Table 1).
Laboratory Analyses The total leukocyte count (WBC)did not differ between the two groups ( P =0.937; Table 1). The total eosinophil count (322.22±276.03/mm 3 ) and eosinophil percentages (4.45%±3.43%) were significantly higher in SAC group compared to the controls ( P <0.001; Table 1). Likewise, the mean erythrocyte volume (MCV) (86.31±6.16 μm 3 ) was significantly elevated in SAC subjects compared to the controls ( P =0.003; Table 1).The tear IgE levels were 3.88±0.48 kU/L and 2.74±0.4 kU/L in SAC and control subjects, respectively. The IgE levels were significantly higher in SAC group than the controls( P =0.042; Table 1). SAC patients demonstrated symptoms including itching, tearing, redness, eyelid swelling, and chemosis at a significantly higher rate compared to the control subjects ( P <0.001; Table 1). 25-OH Vitamin D levels were not significantly different between the two groups ( P =0.501;Table 1). An atopy was observed for 72% of the patient group.In this group, 59.2% of the subjects demonstrated sensitivity to pollen, 17.1% to house dust mites, 6.6% to fungi, and 3.9%to animal dander (cat and cockroach). In the present study,it was also found that 15.6% of the patients demonstrated sensitivity to multiple aeroallergens. In CG, only two patients(2.8%) demonstrated sensitivity to pollen or house dust mites. The results of bivariate analyses suggested a mild positive correlation between total eosinophil count and tearing( r =0.242, P =0.003), itching ( r =0.288, P <0.001), redness( r =0.276, P =0.001) and eyelid swelling ( r =306, P <0.001).There was no significant correlation between serum total IgE level and clinical findings. However, a weak correlation was observed between tear total IgE levels and tearing ( r =0.181, P =0.035) and redness ( r =0.259, P =0.008).
Prenatal and Natal Factors There were no significant difference between SAC and the maternal exposure to cigarette smoking or gestational antibiotic use as well as mode of delivery, and birth weight ( P >0.05; Table 2). Maternal exposure to paracetamol during pregnancy was significantly higher in SAC group compared to the controls ( P <0.001; Table 2).
Postnatal Factors No significant difference was found between SAC and postnatal exposure to paternal or maternal cigarette smoking, owing a pet and drug allergy ( P >0.05;Table 2). The results did not suggest any association between SAC and asthma and allergic rhinitis in parents and siblings( P >0.05; Table 2). There was also no association between SAC and living in the city center, being in a humid environment and modes of heating ( P >0.05; Table 2). The results demonstrated that 97.2% of the control subjects were supplemented with vitamin D during infancy. However, postnatal vitamin D supplementation were significantly reduced in the SAC group and determined to be 85.7% ( P =0.015; Table 2). Likewise, use of vitamin D supplements during infancy were significantly longer in controls compared to the SAC group ( P <0.001).Common asthma (24.3%), allergic rhinitis (73%) and oral allergy syndrome (17.6%) were present in patients with SAC at significantly higher rates compared to the controls ( P <0.001;Table 2). Mothers and siblings of SAC patients demonstrated significantly higher rates of conjunctivitis (5.4% and 5.4%respectively, P =0.047; Table 2). Likewise, fathers of SAC patients exhibited significantly higher rates of allergic rhinitis(14.9%, P =0.003; Table 2). A significantly higher number of SAC patients attended kindergarten compared to the controls(18.3 vs 4.3 respectively, P =0.009; Table 2).
DISCUSSION
In the present study, possible risk factors that play a role in the formation of SAC were evaluated through evaluation of the serum biochemical values, skin allergy tests and performing questionnaires. The results showed that gestational exposure to paracetamol were significantly higher in the SAC group compared to the controls. Likewise, postnatal vitamin D supplementation was significantly shorter in the SAC patients.In the literature, there are many studies that examine the correlation between vitamin D and allergic diseases. It has been proposed that vitamin D has immunomodulatory effects and its deficiency is suggested to play an active role for the onset of allergic and autoimmune diseases [9] . It is thought that the treatment of vitamin D deficiency might change the intensity of allergic diseases. Therefore, it is important to demonstrate the association between the allergic diseases and vitamin D deficiency. Dadaci et al [12] evaluated the serum vitamin D levels of patients and found that the plasma vitamin D levels of patients with SAC were significantly lower than those of the CG. It was the first in the literature to show that SAC patients have decreased vitamin D levels. Therefore, they concluded that vitamin D replacement could be implemented in addition to classical treatment in SAC patients with insufficient vitamin D levels [12] . In the literature, no correlation has been demonstrated between the treatment of vitamin D deficiency and the intensity of allergic conjunctivitis. However,treatment of vitamin D deficiency in asthma patients reducedthe frequency of asthma attacks [13] . As opposite to the findings of Dadaci et al [12] , in the present study, serum vitamin D levels were similar between the two groups. However, it was found that patients who were not supplemented with vitamin D during the postnatal period demonstrated higher rate of SAC.Likewise, the duration of the use of vitamin D supplements during infancy were significantly higher in the control subjects.This information suggests that supplementing vitamin D during infancy, which is the most critical time period for the establishment of immune system, might play an active role for the prevention of allergic conjunctivitis.
Table 2 Prenatal-natal-postnatal risk factors %
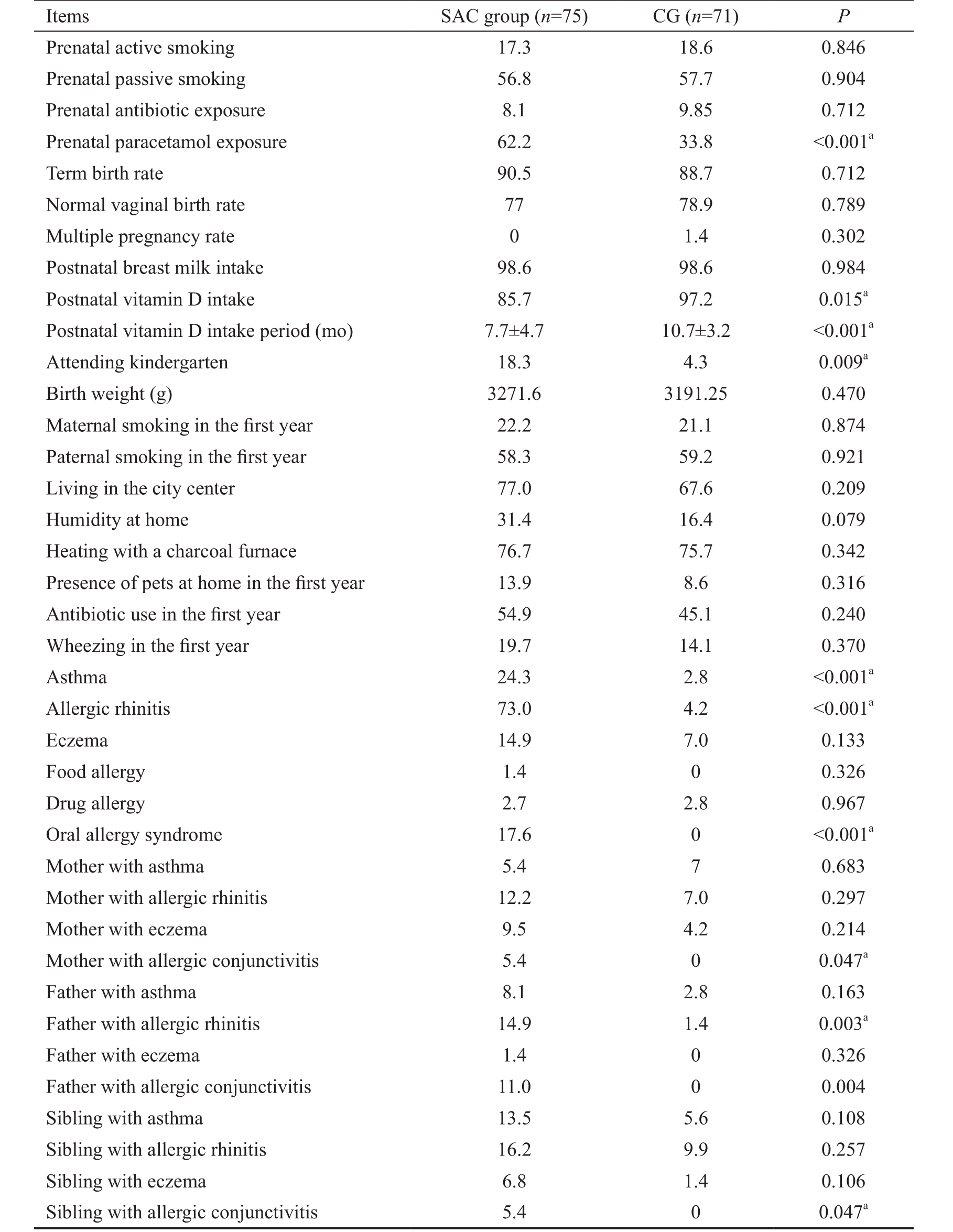
a P <0.05 was accepted as statistically significant.
Items SAC group ( n =75) CG ( n =71) P Prenatal active smoking 17.3 18.6 0.846 Prenatal passive smoking 56.8 57.7 0.904 Prenatal antibiotic exposure 8.1 9.85 0.712 Prenatal paracetamol exposure 62.2 33.8 <0.001 a Term birth rate 90.5 88.7 0.712 Normal vaginal birth rate 77 78.9 0.789 Multiple pregnancy rate 0 1.4 0.302 Postnatal breast milk intake 98.6 98.6 0.984 Postnatal vitamin D intake 85.7 97.2 0.015 a Postnatal vitamin D intake period (mo) 7.7±4.7 10.7±3.2 <0.001 a Attending kindergarten 18.3 4.3 0.009 a Birth weight (g) 3271.6 3191.25 0.470 Maternal smoking in the first year 22.2 21.1 0.874 Paternal smoking in the first year 58.3 59.2 0.921 Living in the city center 77.0 67.6 0.209 Humidity at home 31.4 16.4 0.079 Heating with a charcoal furnace 76.7 75.7 0.342 Presence of pets at home in the first year 13.9 8.6 0.316 Antibiotic use in the first year 54.9 45.1 0.240 Wheezing in the first year 19.7 14.1 0.370 Asthma 24.3 2.8 <0.001 a Allergic rhinitis 73.0 4.2 <0.001 a Eczema 14.9 7.0 0.133 Food allergy 1.4 0 0.326 Drug allergy 2.7 2.8 0.967 Oral allergy syndrome 17.6 0 <0.001 a Mother with asthma 5.4 7 0.683 Mother with allergic rhinitis 12.2 7.0 0.297 Mother with eczema 9.5 4.2 0.214 Mother with allergic conjunctivitis 5.4 0 0.047 a Father with asthma 8.1 2.8 0.163 Father with allergic rhinitis 14.9 1.4 0.003 a Father with eczema 1.4 0 0.326 Father with allergic conjunctivitis 11.0 0 0.004 Sibling with asthma 13.5 5.6 0.108 Sibling with allergic rhinitis 16.2 9.9 0.257 Sibling with eczema 6.8 1.4 0.106 Sibling with allergic conjunctivitis 5.4 0 0.047 a
Paracetamol is an analgesic and antipyretic medicine commonly used by pregnant women. The recent findings indicate a positive correlation between the maternal exposure to paracetamol and the increased incidence of asthma in children [14-15] . Only limited number of studies in the literature investigated the association between the allergic conjunctivitis and postnatal or prenatal paracetamol exposure. However,these studies failed to demonstrate any association [16-18] . In a study by Beasley et al [19] in 2008, an increase in rhinoconjunctivitis and eczema symptoms was observed over time with the use of paracetamol in children aged between 6-7y. Shaheen et al [20] also examined the association between frequent use of paracetamol and asthma in adults. It was determined that the frequent use of paracetamol may contribute to asthma morbidity and rhinitis in adults. In the current study, prenatal paracetamol exposure was significantly higher in the SAC patient group.
Paracetamol’s adverse effect is most likely carried out through decreased level of glutathione leading to increased oxidative stress induced inflammation [21] . Moreover, an antipyretic effect of paracetamol is carried out through the suppression of cyclo-oxygenase pathway favoring the production of prostaglandin E2, which may incline T-helper lymphocytes to a Th2 response. Conversely, such a mechanism suppresses the Th-1 related cytokine release that plays a role for the onset of allergic diseases. Due to increased Th2 response, paracetamol could be involved for the increased prevalence of allergic diseases [20,22] . Our results suggest that maternal paracetamol exposure during pregnancy may play a role in development of SAC. However, there is a need for further extensive research to support this idea.
It was also determined that there was no association between SAC and exposure to maternal smoking, antibiotic use during the pregnancy, the mode of delivery and birthweight.Likewise, no effects was seen in relation to postnatal exposure to maternal and paternal smoking and owing pets at home,eczema, food and drug allergy, living in the city center, being in humid environments, and modes of heating. Although these factors are thought to be predisposing factors for the development of SAC, further extensive research is required to support this idea.
In the literature, it has been mostly shown that attendance to nursery school is related to decreased risk of allergic diseases.However, our results indicate that children who attended kindergarten have a higher risk of SAC. Low number of participants and low rates of participation might have an impact for the results of the current study. Therefore, more studies are required to support this idea.
Of all patients with allergic rhinitis, 30%-71% have allergic conjunctivitis or conjunctival symptoms. Allergic conjunctivitis,by itself, is seen in approximately 6%-30% of the general population [9,23-25] . The prevalence of allergic rhinitis, allergic conjunctivitis, and asthma has increased significantly in the general population. Various studies have investigated the coexistence of these three diseases, particularly the fact that it is seen in developed cities where air pollution is high, supports the link between industrialization and allergic diseases [26-29] .The current study was conducted in an industrialized and developing region and a high rate of allergic diseases were detected, which also supports the results of other studies in literature. The present study also supports that there is an association between SAC and asthma and allergic rhinitis in parents and siblings.
One of the main limitations of our study may be over- or under-reporting due to recollection bias. The number of subjects participating in the study and the retrospective design of the study might be a limitation for the determination of cause and effect relationship.
In conclusion, maternal paracetamol exposure during pregnancy may induce SAC. On the other hand, longer duration of postnatal vitamin D supplementation may reduce the incidence of SAC. The results of the present study also indicate that SAC patients are more likely to have asthma,allergic rhinitis and oral allergy syndrome diseases. Moreover,their relatives also may demonstrate higher rates of allergic diseases. Further studies are required to determine predisposing factors that may lead to the development of SAC.
ACKNOWLEDGEMENTS
We thank Dr. Mustafa Erkoçoğlu for his support finding allergy patients and collecting data. We also thank Dr. Çağri Çamsari and Shawnda M. Çamsari for their technical assistance.
Fundation: Supported by Scientific Research Project Unit of Abant Izzet Baysal University (Project No.: BAP-2016.08.13.1057).
Confilcts of Interest: Doğan Ü, None; Ağca S, None.
REFERENCES
1 Solomon A, Pe’er J, Levi-Schaffer F. Advances in ocular allergy: basic mechanisms, clinical patterns and new therapies. Curr Opin Allergy Clin Immunol 2001;1(5):477-482.
2 Mimura T, Amano S, Funatsu H, Yamagami S, Araie M, Kaji Y, Arimoto A, Ishida Y, Usui T, Okamoto S. Correlations between allergen-specific IgE serum levels in patients with allergic conjunctivitis in spring. Ocul Immunol Inflamm 2004;12(1):45-51.
3 Mimura T, Yamagami S, Amano S, Funatsu H, Arimoto A, Usui T,Ono K, Araie M, Okamoto S. Allergens in Japanese patients with allergic conjunctivitis in autumn. Eye (Lond) 2005;19(9):995-999.
4 Ono SJ, Abelson MB. Allergic conjunctivitis: update on pathophysiology and prospects for future treatment. J Allergy Clin Immunol 2005;115(1):118-122.
5 Bielory L. Allergic diseases of the eye. Med Clin North Am 2006;90(1):129-148.
6 Rosario N, Bielory L. Epidemiology of allergic conjunctivitis. Curr Opin Allergy Clin Immunol 2011;11(5):471-476.
7 Adams JS, Hewison M. Unexpected actions of vitamin D: new perspectives on the regulation of innate and adaptive immunity. Nat Clin Pract Endocrinol Metab 2008;4(2):80-90.
8 Feskanich D, Ma J, Fuchs CS, Kirkner GJ, Hankinson SE, Hollis BW,Giovannucci EL. Plasma vitamin D metabolites and risk of colorectal cancer in women. Cancer Epidemiol Biomarkers Prev 2004;13(9):1502-1508.
9 Frieri M, Valluri A. Vitamin D deficiency as a risk factor for allergic disorders and immune mechanisms. Allergy Asthma Proc 2011;32(6):438-444.
10 Allen KJ, Koplin JJ, Ponsonby AL, Gurrin LC, Wake M, Vuillermin P,Martin P, Matheson M, Lowe A, Robinson M, Tey D, Osborne NJ, Dang T, Tina Tan HT, Thiele L, Anderson D, Czech H, Sanjeevan J, Zurzolo G, Dwyer T, Tang ML, Hill D, Dharmage SC. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J Allergy Clin Immunol 2013;131(4):1109-1116.
11 Abelson MB, Chambers WA, Smith LM. Conjunctival allergen challenge. A clinical approach to studying allergic conjunctivitis. Arch Ophthalmol 1990;108(1):84-88.
12 Dadaci Z, Borazan M, Kiyici A, Oncel Acir N. Plasma vitamin D and serum total immunoglobulin E levels in patients with seasonal allergic conjunctivitis. Acta Ophthalmol 2014;92(6):e443-e446.
13 Solidoro P, Bellocchia M, Aredano I, Mattei A, Pivetta E, Patrucco F,Boita M, de Blasio F, Brussino L, Rolla G, Bucca C. Asthmatic patients with vitamin D deficiency have decreased exacerbations after vitamin replacement. Nutrients 2017;9(11):1234.
14 Magnus MC, Karlstad Ø, Håberg SE, Nafstad P, Davey Smith G,Nystad W. Prenatal and infant paracetamol exposure and development of asthma: the Norwegian Mother and Child Cohort Study. Int J Epidemiol 2016;45(2):512-522.
15 Cheelo M, Lodge CJ, Dharmage SC, Simpson JA, Matheson M,Heinrich J, Lowe AJ. Paracetamol exposure in pregnancy and early childhood and development of childhood asthma: a systematic review and meta-analysis. Arch Dis Child 2015;100(1):81-89.
16 Han YY, Forno E, Badellino HA, Celedón JC. Antibiotic use in early life, rural residence, and allergic diseases in argentinean children. J Allergy Clin Immunol Pract 2017;5(4):1112-1118.e2.
17 Garcia-Marcos L, Robertson CF, Ross Anderson H, Ellwood P,Williams HC, Wong GW, Group IPTS. Does migration affect asthma,rhinoconjunctivitis and eczema prevalence? Global findings from the international study of asthma and allergies in childhood. Int J Epidemiol 2014;43(6):1846-1854.
18 Moyes CD, Clayton T, Pearce N, Asher MI, Ellwood P, Mackay R,Mitchell E, Pattemore P, Stewart AW, Crane J. Time trends and risk factors for rhinoconjunctivitis in New Zealand children: an International Study of Asthma and Allergies in Childhood (ISAAC) survey. J Paediatr Child Health 2012;48(10):913-920.
19 Mimura T, Usui T, Yamagami S, Miyai T, Amano S. Relationship between total tear IgE and specific serum IgE in autumnal allergic conjunctivitis. Cornea 2013;32(1):14-19.
20 Shaheen SO, Sterne JA, Songhurst CE, Burney PG. Frequent paracetamol use and asthma in adults. Thorax 2000;55(4):266-270.
21 Varner AE, Busse WW, Lemanske RF Jr. Hypothesis: decreased use of pediatric aspirin has contributed to the increasing prevalence of childhood asthma. Ann Allergy Asthma Immunol 1998;81(4):347-351.
22 Farquhar H, Stewart A, Mitchell E, Crane J, Eyers S, Weatherall M,Beasley R. The role of paracetamol in the pathogenesis of asthma. Clin Exp Allergy 2010;40(1):32-41.
23 Agrawal T, Gupta GK, Agrawal DK. Vitamin D supplementation reduces airway hyperresponsiveness and allergic airway inflammation in a murine model. Clin Exp Allergy 2013;43(6):672-683.
24 Lee JE, Ahn JC, Han DH, Kim DY, Kim JW, Cho SH, Park HW, Rhee CS. Variability of offending allergens of allergic rhinitis according to age:optimization of skin prick test allergens. Allergy Asthma Immunol Res 2014;6(1):47-54.
25 Leonardi A, Castegnaro A, Valerio AL, Lazzarini D. Epidemiology of allergic conjunctivitis: clinical appearance and treatment patterns in a population-based study. Curr Opin Allergy Clin Immunol 2015;15(5):482-488.
26 Ådjers K, Luukkainen A, Pekkanen J, Hurme M, Huhtala H, Renkonen R, Wang Y, Mäkelä MJ, Karjalainen J, Toppila-Salmi S. Self-reported allergic rhinitis and/or allergic conjunctivitis associate with IL13 rs20541 polymorphism in finnish adult asthma patients. Int Arch Allergy Immunol 2017;172(2):123-128.
27 Dobashi K, Akiyama K, Usami A, et al . Japanese guideline for occupational allergic diseases 2014. Allergol Int 2014;63(3):421-442.
28 Murphy K, Gawchik S, Bernstein D, Andersen J, Pedersen MR.A phase 3 trial assessing the efficacy and safety of grass allergy immunotherapy tablet in subjects with grass pollen-induced allergic rhinitis with or without conjunctivitis, with or without asthma. J Negat Results Biomed 2013;12:10.
29 Wheatley LM, Togias A. Clinical practice. Allergic rhinitis. N Engl J Med 2015;372(5):456-463.
Citation: Doğan Ü, Ağca S. Investigation of possible risk factors in the development of seasonal allergic conjunctivitis. Int J Ophthalmol 2018;11(9):1508-1513
Received: 2017-10-10 Accepted: 2018-03-21
DOl: 10.18240/ijo.2018.09.13
Correspondence to: Ümit Doğan. Department of Ophthalmology, Medical Faculty, Abant Izzet Baysal University, Bolu 14280, Turkey. u_dogan@hotmail.com