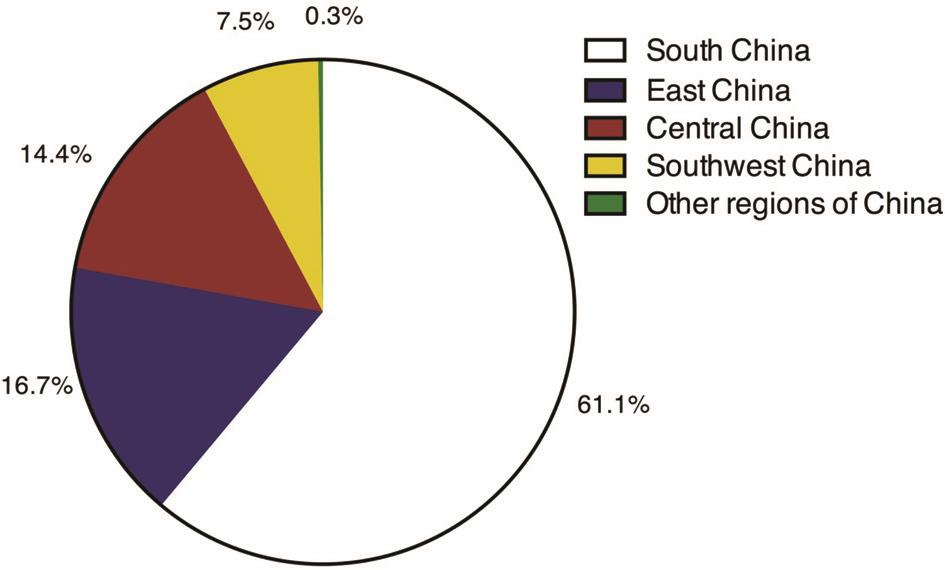
Figure 1 Residences of CEL in-patients from 2006 to 2015.
Guang-Ming Jin 1 , Min Fan 2 , Qian-Zhong Cao 1 , Jun-Xiong Lin 1 , Yi-Chi Zhang 3 , Jian-Qiang Lin 1 ,Yi-Yao Wang 1 , Charlotte-Aimee Young 4 , Dan-Ying Zheng 1
1 State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou 510060, Guangdong Province, China
2 The Third Affiliated Hospital of Sun Yat-sen University-Lingnan Hospital General Internal Medicine, Guangzhou 510000, Guangdong Province, China
3 Department of Ophthalmology, Guangdong Provincial Key Laboratory of Malignant Tumor Epigenetics and Gene Regulation, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou 510000, Guangdong Province, China
4 Department of Ophthalmology, University of California, San Francisco, CA 94115, United States
Congenital ectopia lentis (CEL) is a congenital zonular disease that leads to displacement of the lens from its natural position, with a prevalence of approximately 6 in 100 000 individuals [1] . It usually occurs bilaterally and often associated with inherited connective tissue disorder such as Marfan syndrome, Weill-Marchesani syndrome,homocystinuria and Ehlers Danlos syndrome [2] . According to a national-wide retrospective study in Denmark, 68.2% of the patients with CEL were found to have Marfan syndrome [1] .Dislocation of the lens can cause high refractive error, irregular astigmatism, decreased best corrected visual acuity (BCVA)and monocular diplopia. Other complications of CEL include high myopia, glaucoma, retinal detachment and many other ocular complications [3] . Unfortunately, the lack of guidelines available in the healthcare industry at present makes the treatment of CEL very challenging, particularly in children.Appropriate and timely management should be taken to prevent strabismus, amblyopia and blindness.
Population-based data of CEL can help us better understand the epidemiology current status of management, challenges and future strategies to approach the disease. However, there has been no other large sample sized study about the prevalence and incidence of CEL apart from the Danish national study and Faivre’s study [1,4] . Thus, we decided to conduct a 10-year retrospective study on CEL at Zhongshan Opthalmic Center(ZOC), which is the one of the best and the largest hospitals in southern China to elucidate its demographic characteristics,pathogenetic conditions and treatments in Chinese population.
Subjects This research was designed as a retrospective study.In the database of the Medical Records Department of the ZOC, CEL and ocular abnormalities are coded using the International Statistical Classification of Diseases and Related Health Problems, 10 th Revision (ICD-10). The research studied CEL in-patients younger than 18-years-old who were treated from Jan. 1 st 2006 to Dec. 31 th 2015, at ZOC in China. The cases with the following codes were identified in the records:congenital displaced lens (Q12.1), spherophakia (Q12.4),other congenital malformations of the anterior segment of eye(Q13.8), congenital malformation syndromes predominantly affecting facial appearance (Q87.0), Marfan syndrome(Q87.4), and dislocation of lens (H27.1). Every case record was accepted and reviewed by two independent researchers to confirm the presence of ectopia lentis (EL) in the absence of head trauma, ocular trauma, lens dislocation secondary to tumor or surgical operation.
The age, gender, family medical history, history of general disease, hospitalization time, preoperative ocular examination,and postoperative ocular examination were extracted. Patients were divided into the following 4 groups: less than 3 years old(0-3y), 3 to 6 years old (3-6y), 6 to 12 years old (6-12y), and 12 to 18 years old (12-18y). Most of the medical records included all the necessary information for analysis. Those that did not contain all the required information as mentioned above were excluded from this study.
The study followed the tenets of the Declaration of Helsinki and was approved by the institutional review board of Zhongshan Ophthalmic Center in Sun Yat-sen University (IRB-ZOC-SYSU),Guangzhou, China. As a retrospective study that collected data from the database of the medical records, our study was exempt from participant consent by the IRB-ZOC-SYSU.
Statistical Analysis All of the data were inputted into a Microsoft Excel (Microsoft Corp., Redmond, Washington,USA) data sheet, categorized and analyzed by two of the researchers, and checked reciprocally. Overall, age-specific and sex-specific hospital based prevalence of CEL and its individual characteristics were assessed. Chi-square tests and Mann-Whitney U test were used to compare characteristics between different genders and different age groups. All the data analyses were performed using Stata 12.0 software (Stata crop, College Station, TX, USA).
Based on the data from the Medical Records, 288 308 hospitalizations for various eye diseases were identified during the 10-year study window. Among these hospitalizations,3791 (1.31%) were diagnosed with EL and 437 (0.15%)hospitalizations were diagnosed with CEL. Of these patients,306 were treated surgically for the first time, and the data of these patients were extracted and analyzed.
Figure 1 Residences of CEL in-patients from 2006 to 2015.
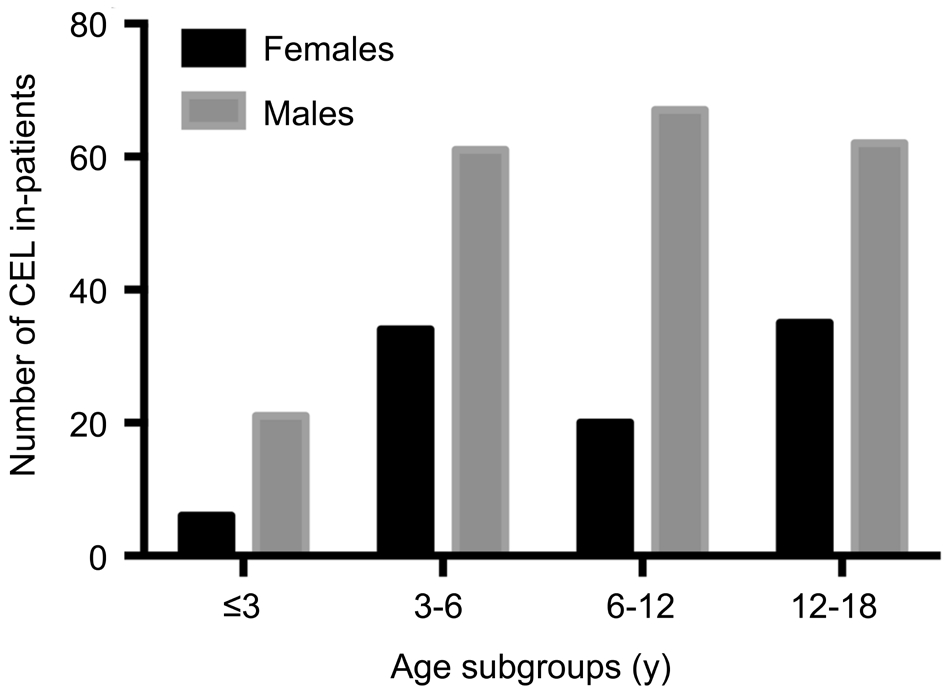
Figure 2 Number of CEL in-patients in different age subgroups.
According to the demographic analysis, patients were from 7 different regions of China (Figure 1). Males accounted for 68.95% of this patient populations (the ratio of males to females was 2.22:1). As shown in Figure 2, the age-group with the lowest proportion of CEL in-patients in both females and males is patients 0-3 years old, at 6.32% and 9.95%,respectively. The age-group with the highest proportion of CEL in-patients in females and males is 12-18 (36.84%)and 6-12 years old (31.75%), respectively. There were no significant differences in the gender ratio between the different age subgroups ( P =0.123).
The characteristics of these patient population were shown in Table 1. Totally 15.36% (47/306) of the CEL patients have a family history of EL and 2.61% (8/306) CEL patients had a systemic medical history of cardiac disease or skeletal abnormality. The 30.39% (93/306) CEL patients had a history of other ocular diseases such as high myopia or retinal detachment. With regard to surgeries, more than two-thirds of the CEL in-patients (250/306, 81.70%) underwent lens extraction with primary intraocular lens (IOL) implantation,while the remaining 18.30% (56/306) of patients received lens extraction surgeries without IOL implantation. The largest proportion of patients who underwent lens extraction surgeries without IOL implantation were patients from the 12-18 years old age group (26/97, 26.80%).
Table 2 showed the visual acuity of the study population before surgery. A number of patients were at very young ageand visual acuity could not be precisely determined, and they were classified as “undetermined” or “unspecified”. As a whole, only 6.21% (19/306) of CEL patients experienced mild or no visual impairment according to presenting visual acuity(PVA) and 10.13% (31/306) experienced mild or no visual impairment according to BCVA measurements. The proportion of CEL patients with mild or no visual impairment using PVA was 0 in 0-3 years old age-group and 9.28% in 12-18 years old age-group. Nonetheless, both BCVA and PVA parameters illustrated that the proportion of CEL patients with mild or no visual impairment increased with age.
Table 1 Age-specific characteristics of CEL in-patients included n (%)
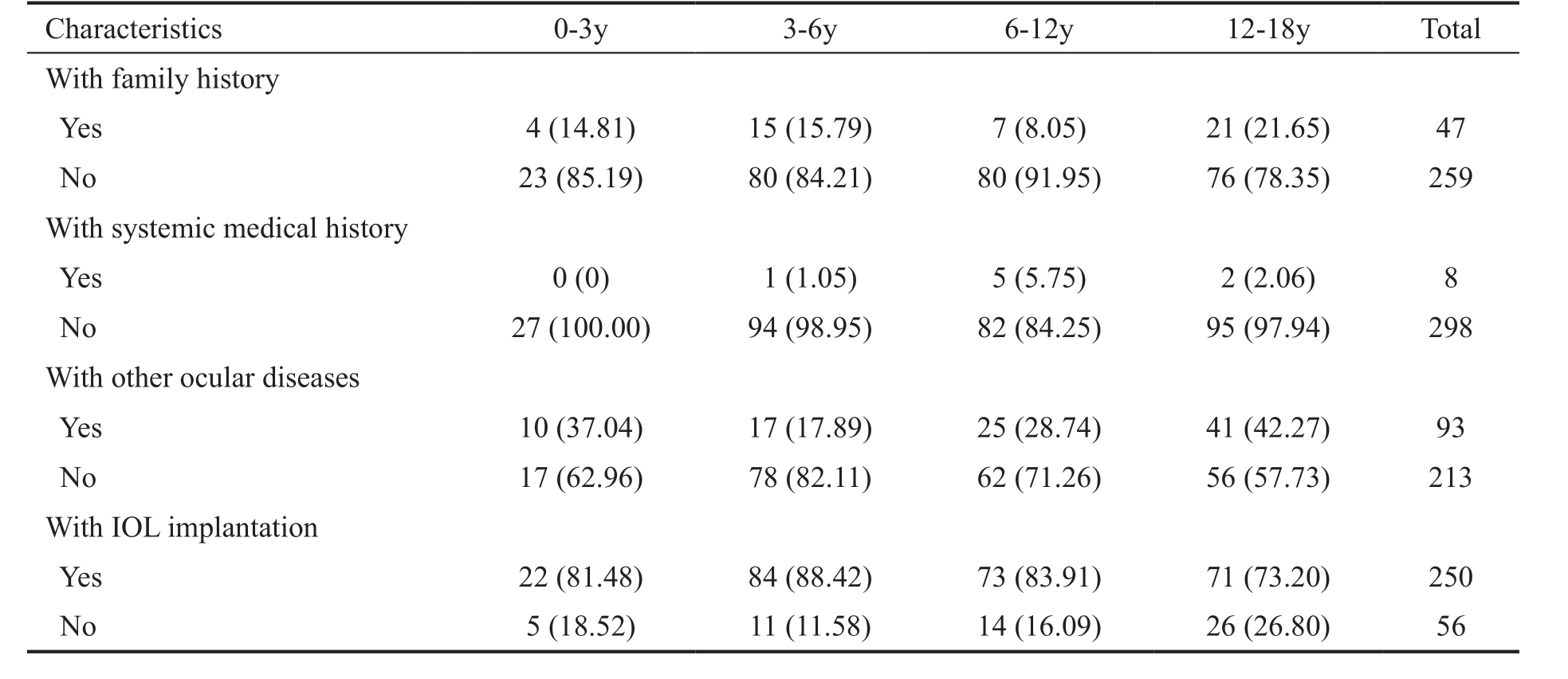
Table 2 Age-specific visual ability distribution of involved eyes in CEL in-patients before surgery n (%)
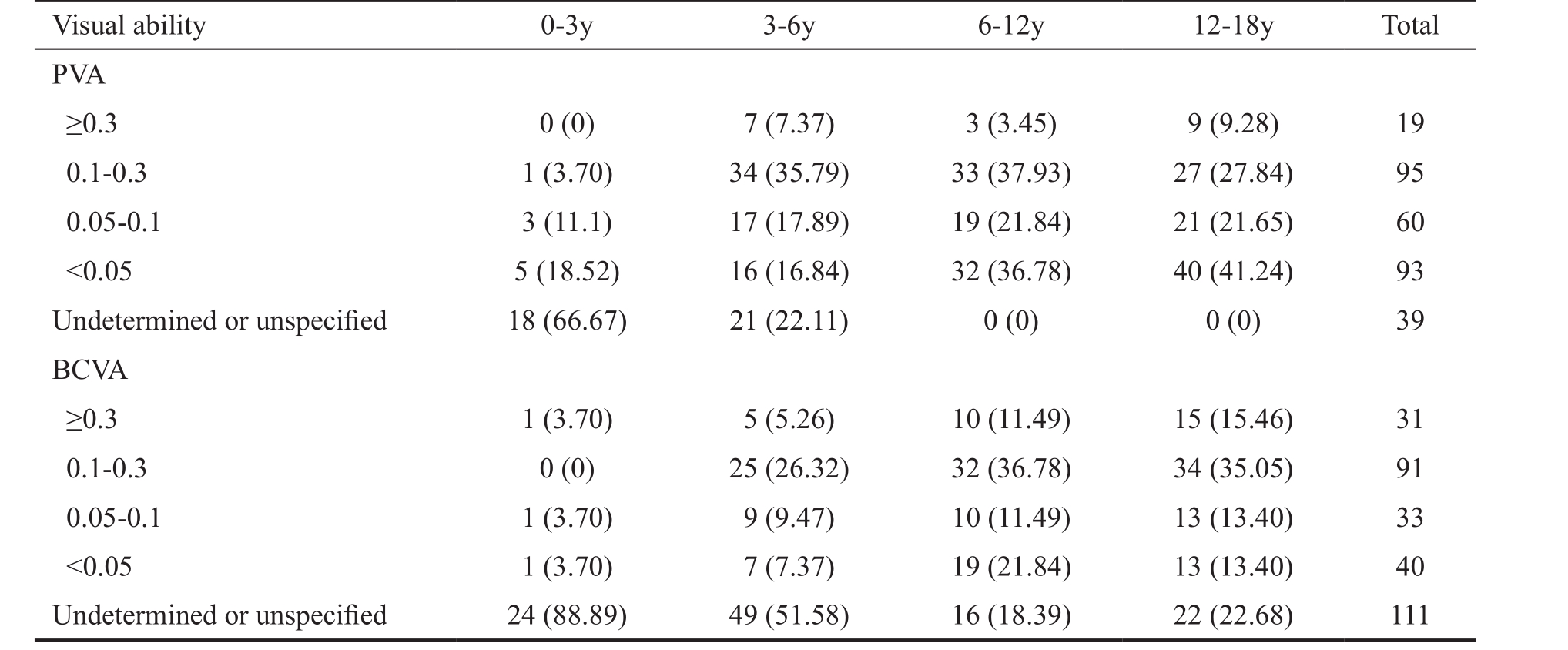
PVA: Presenting visual acuity; BCVA: Best corrected visual acuity.
Among 283 308 hospitalizations, 3791 were diagnosed with EL while 437 of them were diagnosed with CEL. The hospital based prevalence of EL and CEL among ZOC patients during the study period was 1.34% and 0.15%, respectively, with a significant difference ( P <0.05) between boys and girls.However, the ratio of CEL to EL, CEL in-patients ≤6 years old between boys and girls were statistically insignificant( P >0.05), as shown in Table 3.
Figure 3 shows the 10-year overview of the hospital based prevalence and treatment of CEL. The results reveal upward trends in both the number and the hospital based prevalence of CEL in this 10-year study period, but a reduction in the age at surgery.
EL is commonly seen in connective tissue disorders, such as Marfan and Weill-Marchesani syndrome and other conditions can cause subluxation or dislocation of the crystalline lens of the eye. It has been a real clinical dilemma for most ophthalmologists because of the timing for treatment and the variations in vision impairment that these patients can have [5] . Although CEL constitutes only a small proportion of these cases, it has been one of the primary causes of treatable childhood visual impairment [6-8] . As a rare disease, there is no unified standard regarding the timing of surgery for CEL. It is generally considered that when CEL seriously impairs vision and quality of life of the pediatric patient and conservative treatment has been ineffective, surgical intervention shouldbe adopted. Data on epidemiology and characteristics of CEL are critical for improving management strategies for this challenging condition, but many previous studies were conducted with small sample sizes and had focused on the clinical treatments and characteristics of CEL instead of the overall aggregate prevalence [9-11] . This cross-sectional investigation reported the hospital based prevalence of CEL in China from 2006-2015 and the proportion of CEL patients among the total in-patient population in ZOC. We also found that there was a higher prevalence of CEL among boy compared to girl ( P <0.001), and more than 30% of all CEL patients experienced other ocular disease such as glaucoma,high myopia, and retinal detachment. Only 6.21% (19/306) of the patients achieved a PVA that was equal to or better than 0.3, which means that only a few of them were without visual impairment or with mild visual impairment. This 10-year overview also revealed an upward trend in both the number of cases and the hospital based prevalence of CEL, as well as a reduction in age at surgery. Over the 10 years, the number of CEL patients hospitalized in ZOC increased from 18 to 72 per year, and the hospital based prevalence of CEL increased from 8.60/10 000 to 18.10/10 000. The results showed that the average age at surgery of CEL patients decreased from 9.00 to 7.60 years old. Conducted at the largest and most recognized ophthalmic center in southern China [12-13] , the current study may reflect the prevalence of CEL in a broader population, and it could provide an important reference for the development of health policies for the prevention of this debilitating disease in children before any national epidemiological data becomes available.
Table 3 Hospital-based prevalence of CEL
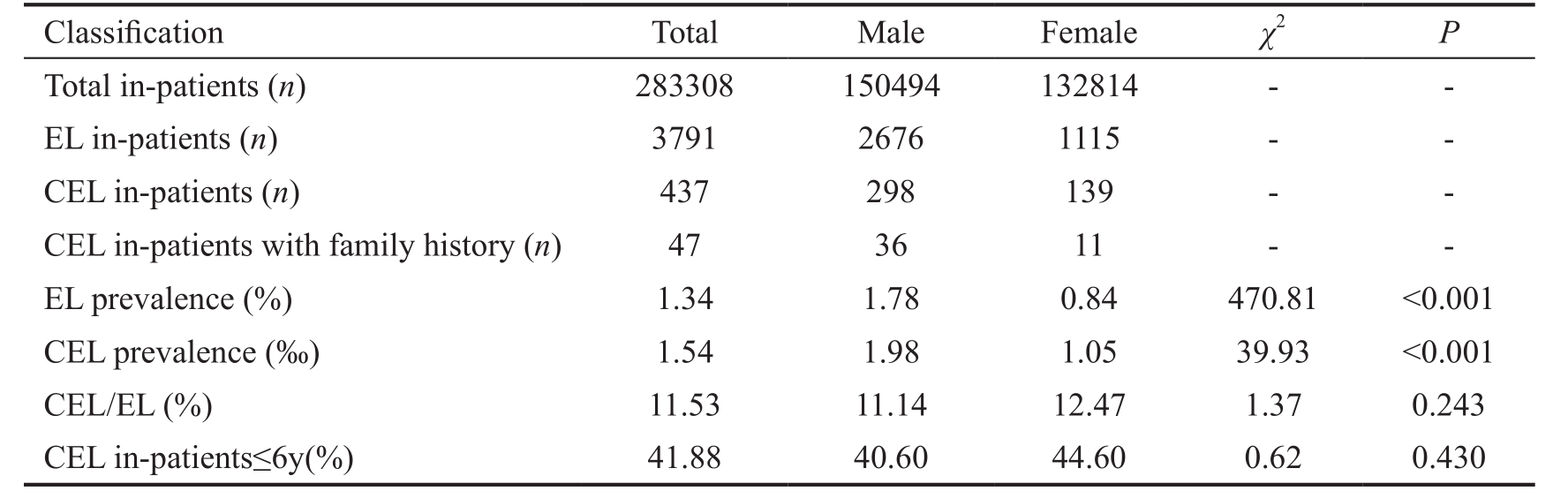
EL: Ectopia lentis; CEL: Congenital ectopia lentis.
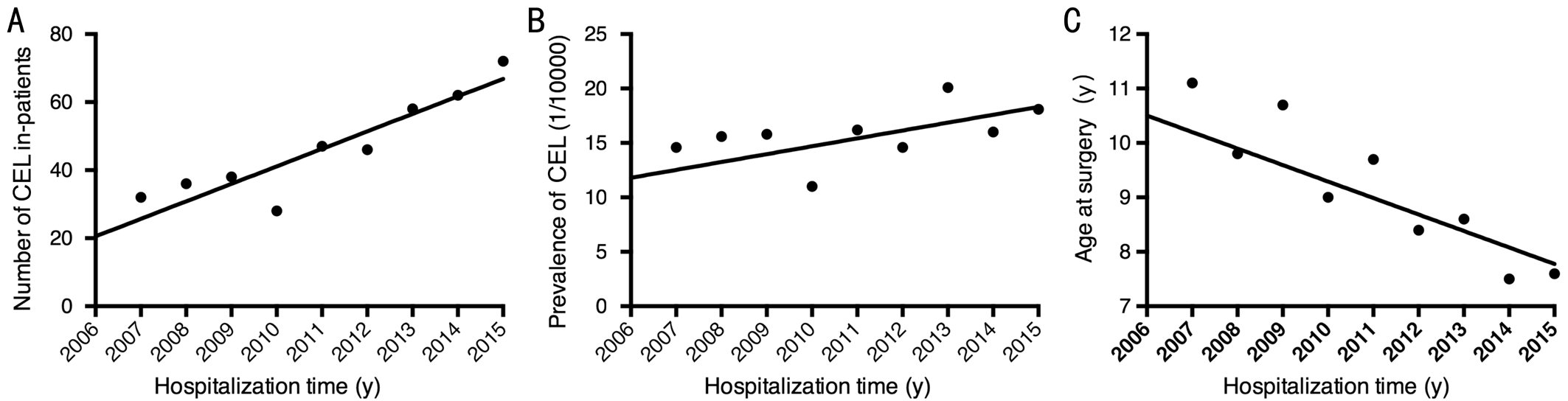
Figure 3 Trends and treatment of CEL in the past 10y The number of CEL in-patients (A) and the incidence of CEL (B) increased during the 10-year period. The age at surgery was decreased during the past decade(C).
To our knowledge, there has no any published reports on epidemiology of CEL in China and few directly comparable prevalence figures are available in the world. Previous study has reported that CEL was found in about 60% of Marfan patients [14] , and the estimated prevalence of Marfan syndrome in USA is approximately 10/100 000 [15] . Additionally, it has been demonstrated that Marfan syndrome, Weill-Marchesani syndrome and homocystinuria account for about 75% of primary lens dislocations, with Marfan syndrome being the most common cause [16-17] . This would indicate a calculated overall prevalence of CEL of 8/100 000, a result that is similar to another study performed in Denmark where the prevalence of CEL was approximately 6.40/100 000 [1] . In the current large sample size, cross-sectional study, the results show that CEL patients accounted for 0.15% of the total in-patients.Although this hospital based prevalence rate does not exactly reflect the national prevalence rate, it can partially reflect the epidemiological condition of this incapacitating disease in Chinese children. Furthermore, we found that the ratio of males to females among the children with CEL was 2.22:1, which was much greater than the gender ratio (male: female=1.05:1)recorded in the sixth national census data of China. The high proportion of males with CEL may be attributed to genderrelated genetic mechanisms or to traditional son preferences in China, although the exact reasons remain unclear and will require further investigation [18] . The rising number and hospital based prevalence of CEL over the 10y may also reflect the greater health consciousness among the Chinese people.
Due to the debilitating nature of this disease, early diagnosis and treatment are extremely important in preventing CEL patients from developing irreversible visual impairment. In this study, the average age for surgery was 9.24±4.83y, and patients 12-18 years old accounted for 31.70% of the study population which suggests that delayed referrals to the hospital and late treatment can be very common in China, which adversely affects the prognosis of CEL in China. However,the downward trend of the average age of CEL patients receiving surgery over the 10y is very encouraging. This may be attributed to increased awareness of this rare disease in China [19] , improvement of treatment techniques [20-21] as well as the increased knowledge of early treatments for CEL among parents [22] .
The limitations of our study should be noted. Firstly, only the surgical patients at the largest ophthalmic center in southern China were included in the study, thus it cannot provide a complete representation of the Chinese population. Despite the limitation, the results of this large sample size study has yielded valuable information on the trends and characteristics of CEL that was previously not as well understood.
In summary, this study presents the trends and characteristics of CEL in a large cohort of surgical patients in southern China.The increasing number and hospital based prevalence of CEL,as well as the reduction of the age at surgery illustrated in this study possibly reflects the improvement of health care system in China. The information and results of the study can potentially be useful for the development of preventative and management strategies for this disease.
ACKNOWLEDGEMENTS
Foundations: Supported by Medical Scientific Research Foundation of Guangdong Province, China (No.A2015490); Science and Technology Planning Project of Guangdong Province, China(No.2014A020212106).
Conflicts of Interest: Jin GM, None; Fan M, None; Cao QZ, None; Lin JX, None; Zhang YC, None; Lin JQ, None; Wang YY, None; Young CA, None; Zheng DY, None.
REFERENCES
1 Fuchs J, Rosenberg T. Congenital ectopia lentis. A Danish national survey. Acta Ophthalmol Scand 1998;76(1):20-26.
2 Sadiq MA, Vanderveen D. Genetics of ectopia lentis. Semin Ophthalmol 2013;28(5-6):313-320.
3 Nemet AY, Assia EI, Apple DJ, Barequet IS. Current concepts of ocular manifestations in Marfan syndrome. Surv Ophthalmol 2006;51(6):561-575.
4 Faivre L, Collod-Beroud G, Loeys BL, et al . Effect of mutation type and location on clinical outcome in 1,013 probands with Marfan syndrome or related phenotypes and FBN1 mutations: an international study. Am J Hum Genet 2007;81(3):454-466.
5 Guo S, Khan AO, Lenhart P, DeRespinis P. Options in the management of reduced vision in a case of ectopia lentis. J Pediatr Ophthalmol Strabismus 2015;52(5):262-264.
6 Moreno-Montañés J, Sainz C, Maldonado MJ. Intraoperative and postoperative complications of Cionni endocapsular ring implantation. J Cataract Refract Surg 2003;29(3):492-497.
7 Ahmed II, Cionni RJ, Kranemann C, Crandall AS. Optimal timing of capsular tension ring implantation: Miyake-Apple video analysis. J Cataract Refract Surg 2005;31(9):1809-1813.
8 Dureau P. Pathophysiology of zonular diseases. Curr Opin Ophthalmol 2008;19(1):27-30.
9 Lam DS, Young AL, Leung AT, Rao SK, Fan DS, Ng JS. Scleral fixation of a capsular tension ring for severe ectopia lentis. J Cataract Refract Surg 2000;26(4):609-612.
10 Konradsen T, Kugelberg M, Zetterström C. Visual outcomes and complications in surgery for ectopia lentis in children. J Cataract Refract Surg 2007;33(5):819-824.
11 Kim EJ, Berg JP, Weikert MP, Kong L, Hamill MB, Koch DD, Yen KG. Scleral-fixated capsular tension rings and segments for ectopia lentis in children. Am J Ophthalmol 2014;158(5):899-904.
12 Dolgin E. The myopia boom. Nature 2015;519(7543):276-278.
13 Chan CC, Liu MM, Tsai JC. The first Western-style hospital in China. Arch Ophthalmol 2011;129(6):791-797.
14 Maumenee IH. The eye in the Marfan syndrome. Trans Am Ophthalmol Soc 1981;79:684-733.
15 Pyeritz RE. The Marfan syndrome. Am Fam Physician 1986;34(6):83-94.
16 Spaeth GL, Winston Barb G. Prevalence of homocystinuria among the mentally retarded: evaluation of a specific screening test. Pediatrics 1967;40(4):586-589.
17 Cross HE. Differential diagnosis and treatment of dislocated lenses. Birth Defects Orig Artic Ser 1976;12(3):335-346.
18 Lin H, Yang Y, Chen JJ, et al . Congenital cataract: prevalence and surgery age at Zhongshan Ophthalmic Center (ZOC). PLoS One 2014;9(7):e101781.
19 Lin H, Long E, Chen W, Liu Y. Documenting rare disease data in China. Science 2015;349(6252):1064.
20 Hsu HY, Edelstein SL, Lind JT. Surgical management of non-traumatic pediatric ectopia lentis: a case series and review of the literature. Saudi J Ophthalmol 2012;26(3):315-321.
21 Simon MA, Origlieri CA, Dinallo AM, Forbes BJ, Wagner RS, Guo S. New management strategies for ectopia lentis. J Pediatr Ophthalmol Strabismus 2015;52(5):269-281.
22 Lin HT, Luo LX, Chen WR, Liu YZ. Eye health is everyone’s responsibility: China’s first Western-style eye hospital improves in the prevention of blindness. Int J Ophthalmol 2012;5(5):638-640.
Citation: Jin GM, Fan M, Cao QZ, Lin JX, Zhang YC, Lin JQ, Wang YY, Young CA, Zheng DY. Trends and characteristics of congenital ectopia lentis in China. Int J Ophthalmol 2018;11(9):1545-1549
Received: 2018-02-12 Accepted: 2018-06-28
DOl: 10.18240/ijo.2018.09.19
Abstract · AlM: To elucidate the trends and characteristics of congenital ectopia lentis (CEL) in southern China.· METHODS: CEL patients from China admitted to Zhongshan Ophthalmic Center (ZOC) from January 2006 to December 2015 were recruited in our study. Residence,gender, hospitalization time, age at surgery, and the presence of other ocular abnormalities and system disease were statistically analyzed in different subgroups.· RESULTS: Four hundred and thirty-seven hospitalizations(306 in-patients) diagnosed with CEL from a total of 283 308 hospitalizations were identified, which accounted for 0.15%of the total in-patients. Of the identified CEL in-patients,the total ratio of boys to girls was 2.22:1. Based on a subgroup analysis according to age, patients aged 12-18 years old constituted the highest proportion (31.70%) of all hospitalized CEL patients, and those 0-3 year old constituted the lowest proportion (8.82%) of the total number. The number of CEL increased from 18 to 72 and the hospital based prevalence increased from 8.60% to 18.10% from 2006 to 2015, and the average age at surgery decreased from 9 years old in 2006 to 7.6 years old in 2015.· CONCLUSlON: The results reveal upward trends in both the number of CEL hospitalizations and hospital based prevalence of CEL in this 10-year study period, but a reduction in the age at surgery, which may reflect the increase of public awareness of children’s eye care in China.· KEYWORDS: congenital ectopia lentis; epidemiology;characteristics; China
Correspondence to: Dan-Ying Zheng. State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yatsen University, Guangzhou 510060, Guangdong Province,China. zhengdyy@163.com
Co-first authors: Guang-Ming Jin, Min Fan and Qian-Zhong Cao