How to improve lranians’ vision health: on the national policy of preventing lranians’ blindness
Behzad Damari1, Alireza Mahdavi2, Maryam Hajian3
1Neuroscience Institute, Tehran University of Medical Sciences, Tehran 1416833481, Iran
2Ministry of Health and Medical Education, Tehran 1467664961, Iran
3Minimally Invasive Surgery Research Center, Iran University of Medical Sciences, Tehran 1445613113, Iran
Abstract● AlM: To review vision health situation of lranian community,analyze its determinants, and discuss the adopted improvement strategies by the lran Ministry of Health and Medical Education (MOHME).● METHODS: This was a rapid situation analysis with a qualitative approach in three parts of recognition, orientation and implementation. The data were gathered via review of upstream documents, national and international experiences, and experts and stakeholders’ opinions.● RESULTS: Eradicating trachoma, increasing human resources, increasing educational and research centers and promotion of ophthalmic technologies were important achievements in the field of vision health in lran. Through these achievements, it seemed that the pattern of causes of blindness and low vision was similar to that of the developed countries. However, the review of lranians’ vision health indicators showed that a considerable percent of the blindness and low vision was avoidable through a national program demanding 3 types of interventions in social determinants of health (SDH),community education, and increasing the access to health care services by integrating the necessary services in primary health care system.● CONCLUSlON: Managing the issue requires attentions from a national committee for preventing blindness with participation of all stakeholders, implementing a national survey on vision health, preparation of the primary level health centers including employment and education of community health workers (Behvarzes), optometrists and general practitioners, fair distribution of specialized human resources and establishing at least one specialized center in each province for referring patients from the primary levels.
INTRODUCTION
W orld Health Organization (WHO) estimate for 2012 shows that about 285 million people suffered vision disorders worldwide; of whom 39 million were blind. In 2010,82% of the blind and 65% of patients with moderate or severe vision disorders were over 50 years old. Vision disorders and blindness are more prevalent among the poor and women.WHO report, however, shows that 19 million out of 285 million patients with vision disorders are children. The 60%of those children suffer refractive errors which is not easily correctable[1].
Vision disorders affects the quality of life. Results of a study have shown that in different grades of age-related macular degeneration (AMD), patients have a 75% to 96% more disappointing concept about losing quality of life than that their physicians have[2]. Losing vision has a negative effect on the job, home life, daily activities, hobbies and social participation of patients. Losing vision means missing opportunities,independency and credit, in addition of losing job and suffering from isolation. Many need help for their daily works.They usually do not have access to vision rehabilitation and many of them suffer poverty[3]. Vision disorders increase the difficulty of daily works as two times normal, decreases social functions as half, increases possibility of falling as two times,increases possibility of depression as three times, and increases possibility of hip fracture as four times[3]. It means that these patients are really vulnerable and their care and support strategy should be changed[2]. Canada has estimated the direct economic cost of vision disorders as 2.7 to 2.9$ billion for year 2006. Considering the indirect costs for treating fractures,depression, etc. the figure reaches to $7.9 billion. Thus, vision disorders are in the 9th place of costly diseases, higher than gastrointestinal and endocrine (including diabetes) diseases, as well as infectious and parasitic ones[3]. Researchers emphasize that economic costs of vision disorders should be considered by policy makers since vision disorders are restricting factors for economic development, even in the most developed countries[2].
Table 1 Preventing interventions for reducing incidence and prevalence of eye diseases
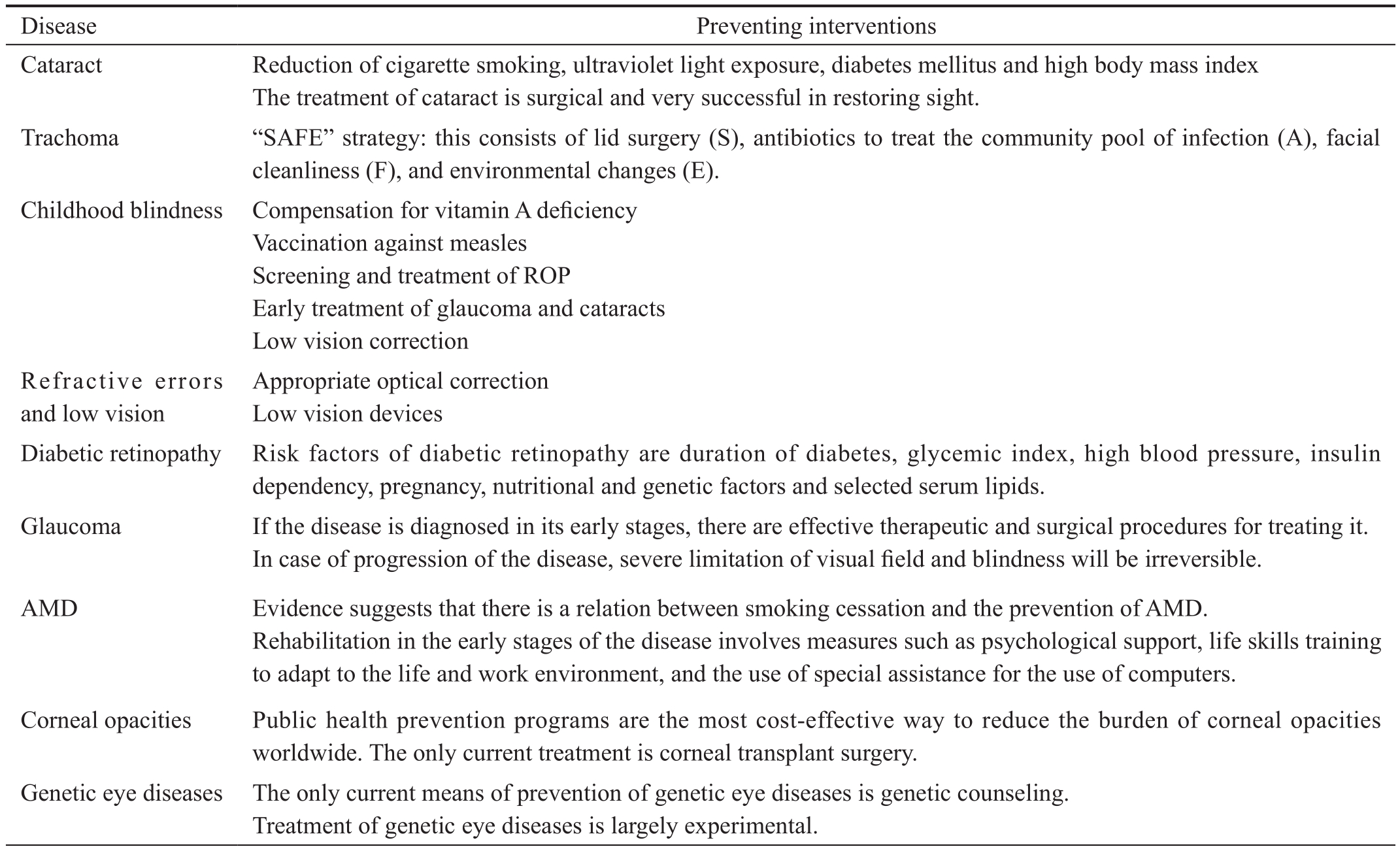
ROP: Retinopathy of prematurity; AMD: Age-related macular degeneration.
Disease Appropriate optical correction Low vision devices Diabetic retinopathy Risk factors of diabetic retinopathy are duration of diabetes, glycemic index, high blood pressure, insulin dependency, pregnancy, nutritional and genetic factors and selected serum lipids.Glaucoma If the disease is diagnosed in its early stages, there are effective therapeutic and surgical procedures for treating it.In case of progression of the disease, severe limitation of visual field and blindness will be irreversible.AMD Evidence suggests that there is a relation between smoking cessation and the prevention of AMD.Rehabilitation in the early stages of the disease involves measures such as psychological support, life skills training to adapt to the life and work environment, and the use of special assistance for the use of computers.Corneal opacities Public health prevention programs are the most cost-effective way to reduce the burden of corneal opacities worldwide. The only current treatment is corneal transplant surgery.Genetic eye diseases The only current means of prevention of genetic eye diseases is genetic counseling.Treatment of genetic eye diseases is largely experimental.Preventing interventions Cataract Reduction of cigarette smoking, ultraviolet light exposure, diabetes mellitus and high body mass index The treatment of cataract is surgical and very successful in restoring sight.Trachoma “SAFE” strategy: this consists of lid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (F), and environmental changes (E).Childhood blindness Compensation for vitamin A deficiency Vaccination against measles Screening and treatment of ROP Early treatment of glaucoma and cataracts Low vision correction Refractive errors and low vision
In the beginning of 21st century, WHO declared that based on medical findings, more than 75% of blindness cases generally occurred at higher ages (including resulted from cataract,refractive errors, diabetic retinopathy, glaucoma and corneal opacities) are preventable[4-7]. Regarding the population growth rate and increase of life expectancy in different communities,it has been estimated that failure in improving ophthalmologic services will increase the prevalence of vision diseases as almost twice in the world, by year 2020[4] .
Resolution 62.1 was the last resolution of WHO on preventing avoidable blindness cases which emphasizes the integration of Primary Eye Care (PEC) in Primary Health Care (PHC)Services, as a necessary action[8]. One of the main ways for achieving this goal is to develop a national program for preventing blindness. Many countries have organized their vision health improvement strategy based on the advices of WHO and its 2020 plan[2].
At this time, according to the report of WHO, most countries of“East Mediterranean Region Of fice” (EMRO) have developed a program to reduce avoidable vision disorders and provide reliable access to rehabilitation services for patients with vision disorders. WHO considers prevention of blindness as one of the most effective methods for combating the poverty, like vaccination[9]. Initiative of “Vision 2020: the Right to Sight”was formed in the beginning of 1999 by WHO, to establish cooperation among this organization and its partners. The goal of this initiative was to eliminate avoidable blindness all over the world, by 2020. Vision 2020 improves the strategy of integrating PEC in PHC. It emphasizes three priorities:combating the certain diseases, developing human resources,and strengthening structure and technology. Although Vision 2020 is a universal program, its implementation requires willing and action of all countries[10]. In addition, WHO has suggested some preventing interventions for reducing incidence and prevalence of eye diseases, which are presented in Table 1.
The goal of this article is to address the current situation of Iranian’s vision health and to present national solutions for preventing blindness, in the form of a policy paper. Therefore,the results will come up with an operational plan to: 1) address the blindness as a priority problem; 2) start managing and monitoring national preventive programs; and 3) inform researchers, service providers, people and patients of their responsibilities for preventing blindness.
Table 2 Stakeholders’ analysis based on impact level and organizational commitment

MOHME: Iran Ministry of Health and Medical Education.
Groups Stakeholders who are member of steering committee Group one: senior managers and policy makers Undersecretary of Treatment (Department of Clinical Authority, Department of Health Validation)Undersecretary of Public Health (Center for Non-communicable Diseases Management, Center for Network Development, Department of Family Health)Deputy Minister for Policy-Making Affairs at MOHME Organization of Welfare (Undersecretary of Disability Preventing)Department of Health at Ministry of Education Representative of the High Council of Insurance Representative of WHO Group two: researches and the elite Iranian Ophthalmology Scientific Association Iranian Social Medicine Scientific Association Infants Scientific Association Nursery Scientific Association Iranian Optometry Association Group four: people Iranian Blind Association Iranian Diabetes Association Representative of the High Council of Provinces Representative of the Health Commission of Parliament ASHK association (Association of supporting the eye injured patients)Group five: media Representative of the Council of Health Policy-Making at Radio & Television Organization Director of Health Channel of Television Director of Health Radio Editor-in-chief of “SALAMAT” weekly Eye Research Center; Shahid Beheshti University of Medical Sciences (WHO’s collaboration center)National Eye Research Center Ophthalmology scientific hubs (Zahedan and Shahid Behesti Universities of Medical Sciences)Noor Research Center Group three: service providers
MATERIALS AND METHODS
This is a rapid situation analysis with a qualitative approach conducted in three parts of recognition, orientation and implementation. The data were gathered via review of upstream documents, national and international experiences,and experts and stakeholders’ opinions[9-42]
Initially, some stakeholders were identified as the steering committee. For this purpose, two criteria were considered:legal responsibility and in fluence on preventing blindness. The stakeholders were divided into five groups. Representative of each group received a decree from the minister of Health as the member of the steering committee (Table 2).
The participants were interviewed using four distinct questions, as “What is the current situation of Iranian’s vision health?”, “What are the effective factors on the current situation of Iranian’s vision health?”, “What are the improvement interventions?”, and “What are the guarantees for the interventions?”
We considered all principles of a structured interview including assuring representativeness of the stakeholder’s network, preinforming the interviewees, providing the interviewees with evidence-based information about country’s situation, having interview guideline, selecting informed interviewers, acquiring permission for recording the voices of interviewees, immediate transcription of the interviews, and due date classification and analyzing the data after determining the main fields.
The related literature were searched through the databases of PubMed, WHO, and Google Scholar by using keywords“eye health prevention factsheet”, “eye health prevention global report”, “eye prevention global report”, “eye health prevention strategy”, “healthy vision prevention strategy”,“eye prevention strategy”, “blindness prevention”, “blindness prevention program”, “service package blindness prevention”,and “sight loss strategy” from 1980 to 2017.
Regarding validity, the acquired information divided into two categories: 1) media news and reports without strict reliability,from scattered programs on eye health; and 2) documents on situation and process of implementing blindness prevention programs.
These documents were retrieved from websites like WHO and CDC. We reviewed the literature retrieved from Iran Ministry of Health and Medical Education (MOHME) and from the websites of research centers and related undersecretaries of MOHME.
Table 3 Indicators of Iranians’ eye health
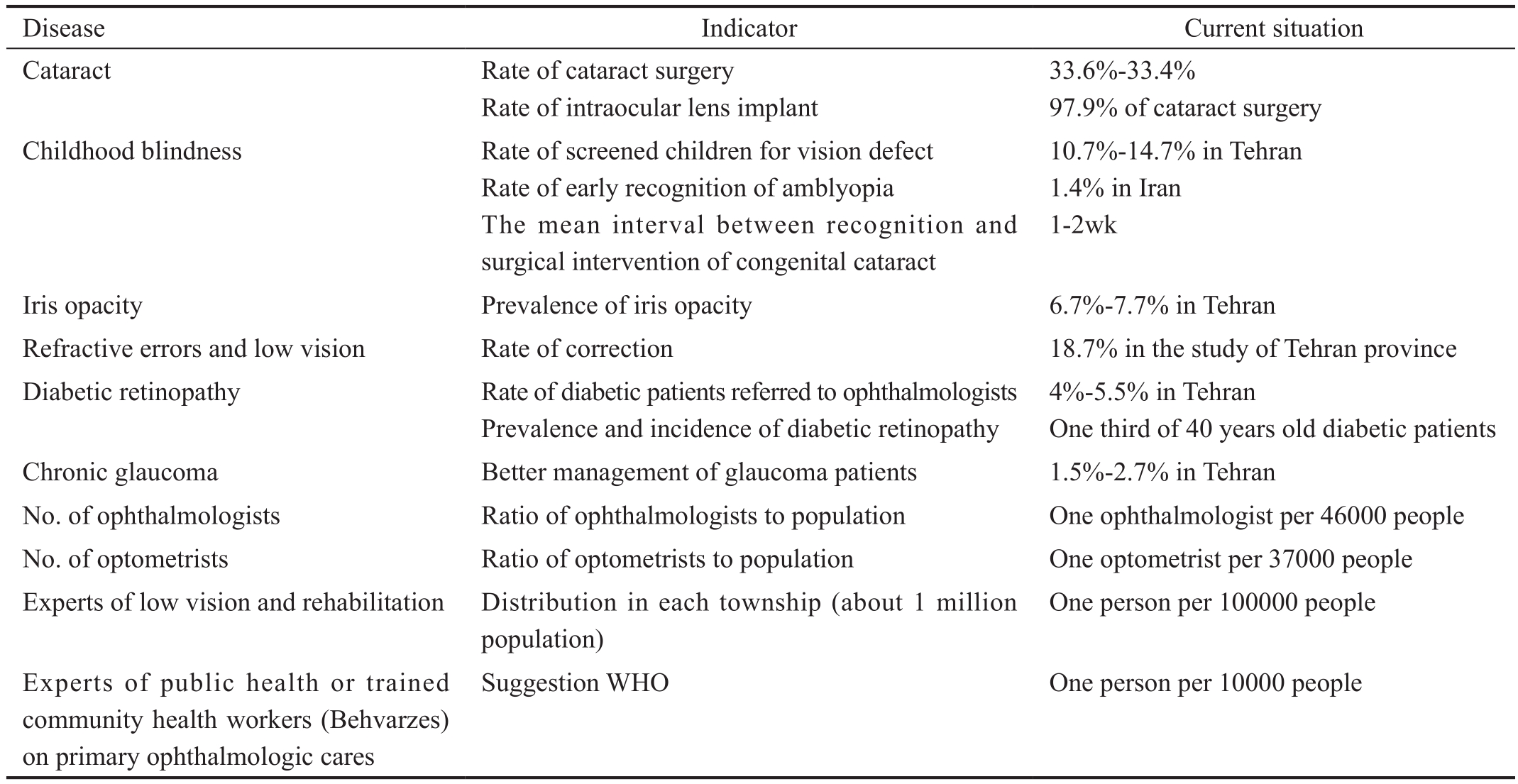
Disease Indicator Current situation Cataract Rate of cataract surgery Rate of intraocular lens implant 33.6%-33.4%97.9% of cataract surgery Childhood blindness Rate of screened children for vision defect Rate of early recognition of amblyopia The mean interval between recognition and surgical intervention of congenital cataract 10.7%-14.7% in Tehran 1.4% in Iran 1-2wk Iris opacity Prevalence of iris opacity 6.7%-7.7% in Tehran Refractive errors and low vision Rate of correction 18.7% in the study of Tehran province Diabetic retinopathy Rate of diabetic patients referred to ophthalmologists Prevalence and incidence of diabetic retinopathy 4%-5.5% in Tehran One third of 40 years old diabetic patients Chronic glaucoma Better management of glaucoma patients 1.5%-2.7% in Tehran No. of ophthalmologists Ratio of ophthalmologists to population One ophthalmologist per 46000 people No. of optometrists Ratio of optometrists to population One optometrist per 37000 people Experts of low vision and rehabilitation Distribution in each township (about 1 million population)One person per 100000 people Experts of public health or trained community health workers (Behvarzes)on primary ophthalmologic cares Suggestion WHO One person per 10000 people
For analyzing the situation and illustration of the structural position, the center for non-communicable disease management was proposed as the national implementation unit for preventing blindness and eye health. Strengths and weaknesses of this unit (in the fields of stewardship, services and resources) were analyzed as the internal environment.The external environment was divided into near (attitude and cooperation of the stakeholders) and far (social, economic,technological, environmental and international factors) and analyzed accordingly. The results of this study is presented in the following three parts: 1) Recognition (described in five sections): information collected on the situation of blindness in impact, outcome and output (from reviewing articles and documents), effective factors on incidence and prevalence of blindness (from comments of stakeholders and published researches), analyzing previous and current interventions program for preventing blindness (from reviewing the collected documents and comments of the elite), reviewing the superior documents (as current support of regulations and policies from preventive programs), and strategic analysis of the strengths, weaknesses, opportunities and threats. 2) Orientation(concluded in three parts): prospects for the prevention of blindness in Iran, future strategic goals and interventions.In the designing and suggesting interventions’ phase, three kinds of strategies (obligatory, promotional and facilitatory)were used and classified. 3) Establishment of administrative necessities, including financial resources, human resources,needed information and needed political support.
RESULTS
Current Situation and Previous Programs Interventions During the past decade, various research have collected the data on prevalence and reasons of blindness and low vision in Iran. In a study on over 50-year-old population of Varamin city which was conducted by Eye Research Center of Shahid Behesti University of Medical Sciences in collaboration with WHO, it was found that about 10% of total population and 16.39% of the studied population suffer blindness or low vision. In that study, the prevalence of two-sided blindness among over 50- and over 60-year-old age groups were 1.3%and 2.07%, respectively. According to other studies, the situation is worse in the deprived areas of the country, so that prevalence of two-sided blindness among over 60-year-old age group in Sistan & Baloochestan and Khorasan provinces were 12.4% and 9.2%, respectively. Table 3 shows indicators of Iranians’ eye health.
Experts in the field of eye diseases believe that cataract,glaucoma, diabetic retinopathy, AMD, vitamin A deficiency,retinopathy of prematurity, keratoconus (especially in the youth), visional nerve related diseases, complications of traumas, fireworks of the festival of the last Wednesday before Nowruz, hypertension, hyperlipidemia, smoking, unhealthy life-style like inactivity and inappropriate diet are the main reasons of blindness and low vision in Iran. In the last five years, most injuries have been resulted from cataract.
Most reasons of blindness are avoidable. Trachoma and Onchocerciasis which are the infections the can lead to blindness, are mostly prevalent in Africa and South-East Asia.These infections are not prevalent in Iran. In Iran, pattern of the reasons of blindness and low vision is like that of the developed countries.
Table 4 Analysis of the system of blindness preventing management and eye health in Iran
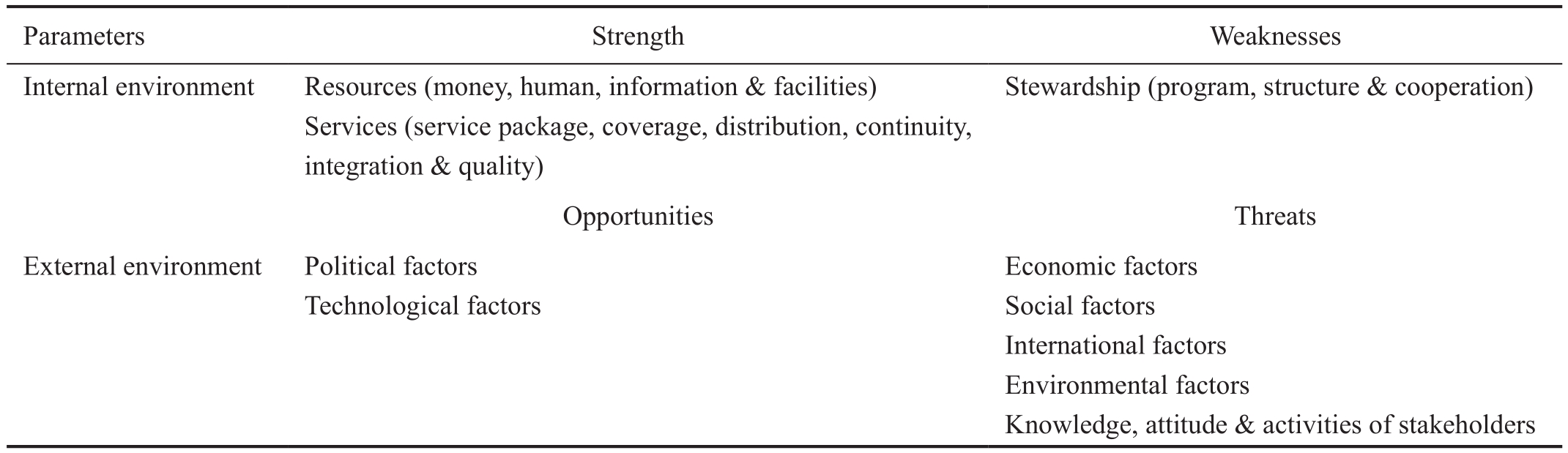
Parameters Strength Weaknesses Internal environment Resources (money, human, information & facilities)Services (service package, coverage, distribution, continuity,integration & quality)Stewardship (program, structure & cooperation)Opportunities Threats External environment Political factors Technological factors Economic factors Social factors International factors Environmental factors Knowledge, attitude & activities of stakeholders
Experts believe that the most important reasons of blindness are the social determinants of health (SDH), lack of accessible services for prevention and treatment, low health literacy of people, lack of referring system and stratification of health service, and inappropriate distribution of specialized ophthalmology human resources. They believe that although Iran has had important achievements in controlling and eliminating trachoma, current programs on preventing blindness are inactive and reactional because of lack of orientation, stratification of health service, referring system and indicators of monitoring and evaluation. The elite believe that joint actions by welfare organization and ministries of Health and Education have helped preventing blindness.
There has been a 3-stage periodic examination program for screening amblyopia among under 6-year-old children (with 71.5% coverage) first by kindergartens’ teachers, second by optometrists, and third by the ophthalmologist (in case of referring by optometrists). Pre-entering examinations at primary schools are done by community health workers(Behvarzes) in rural areas and optometrists in urban areas for finding refracting errors. Examining the infants for retinopathy of prematurity is another current intervention in the country.
One of the achievements of Iran’s health system in the field of vision health is to train enough numbers of eye nurses, at least 1300 ophthalmologists and about 1600 optometrists in the past three decades. Distribution of such nurses, however, has always been a challenge, especially in the deprived areas. Increase of“Cataract Surgical Rate” (CSR) in Iran during the past decade has been known as a preventive intervention, resulted from the increase of the number of eye surgeons. Transmission of ophthalmologic technology through commercial companies of the advanced countries has facilitated treatment of eye diseases,but on the other hand, has increased the treatment costs. The issue is being regularly addressed in various celebrations such as National Vision Day and plenty of seminars and specialized meetings on vision health.
During the past two decades, seven governmental center and one private ophthalmology research center, as well as many NGOs on vision health and blindness have been established in the country. In spite of performing important research on the eye health, we lack for table of prioritized research on this issue in the national level. Of the most important related studies in the country are study of determining loud of eye diseases in Iran, RAAB study in eight points of Iran,screening projects of avoiding children’s blindness, studies of determining prevalence of diabetic retinopathy and cataract surgeries.
Iran has signed the International Commitment Letter of “Vision Health 2020”, and has developed, though not operationalized,the strategic plan of eye health for 2008 to 2011. In Iran,general health policies have been notified to government and parliament by the supreme leader. Those policies emphasized on prevention prior to treatment.
Table 4 shows the analysis of the system of blindness preventing management in Iran. Based on this table, the internal environment is in the strength position, but the external environment suffers from some threats; thus, adopting a maintenance strategy is a practical approach for eye health in Iran’s health system.
Orientation Stakeholders’ opinions, suggested vision,goals, interventions and obligations are categorized in Table 5.The stakeholders believe that the senior managers should be informed of economic, social and psychological effects of blindness on workforce and human capital and integrated prevention of blindness in the primary care system. For this purpose should be defined programs and clinical guidelines in which determine the role of all referring team including community health workers (Behvarzes), optometrist, family physician and ophthalmologists.
These primary services should be planned for preventing the complications of diabetes and glaucoma (through measuring eye internal pressure), vision nerve diseases, and facing to eye trauma and eye redness.
Health literacy level of people on meeting health notes and their general knowledge and attitude toward the right time for following medical visits should be improved through the
media. A reliable data bank which is the base of implementing the national plan of preventing blindness should be developed with cooperation of research centers and MOHME. The responsible sectors should cooperate together for implementing the national screening plan and avoiding of the repetitious works. Improvement of insurance coverage and redefining governmental support for critical illness insurance are among the other suggested interventions.
Table 5 Orientation of Iranians’ blindness prevention by 2020
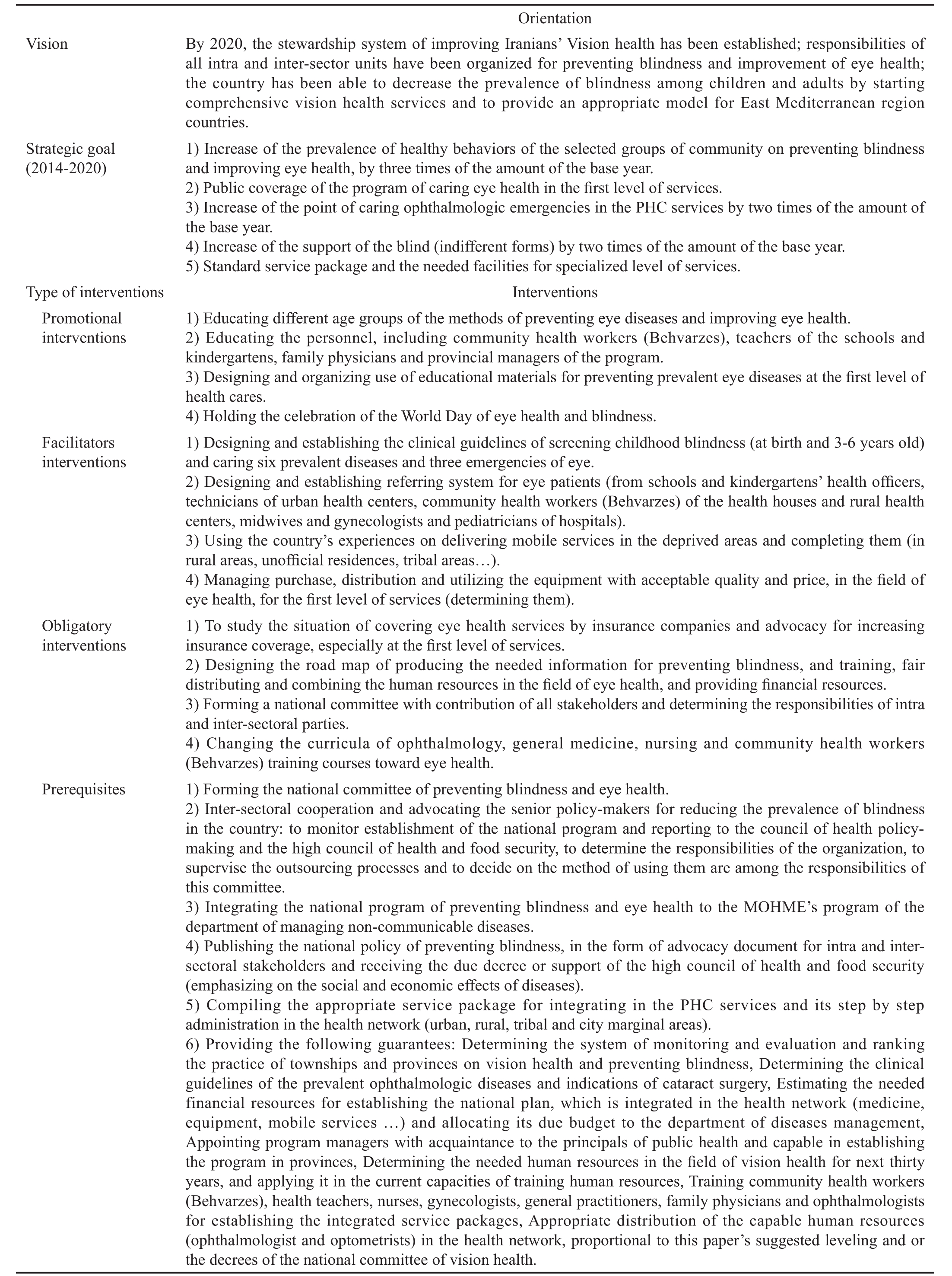
MOHME: Iran Ministry of Health and Medical Education; PHC: Primary Health Care.
?
DISCUSSION
Eradicating trachoma[23], increasing human resources,educational and research centers and promotion of ophthalmic technologies are important achievements in the field of vision health in Iran[25-26].
Thus, current pattern of causes of blindness and low vision is similar to developed countries. However, the review of reports for Iranian vision health indicators showed that a considerable percent of the blindness and low vision is avoidable[4-7] through a national program with intervention in SDH, community education, and increasing the access to health care services by integrating the necessary services in PHC system.
Vision 2020 is a global initiative that aims to eliminate avoidable blindness by the year 2020[1]. The principles of this program are public access and equity, respect for individual rights, evidence-based medicine, considering all life stages,and empowerment of people with visual impairment[9].
According to the WHO’s reports, activities such as problem assessment, recognition of the reasons of vision disorders,development and implementation prevention programs and policies and effectiveness of services are an appropriate solution against visual disorders which relies on three priorities including disease control, human resource development and infrastructure and appropriate technology development[1,9].
Vision 2020 is a global program which its implementation requires suitable collaboration of all countries[10]. In Iran, in tandem with such necessity, a strategic plan was developedthough not yet implemented-by the Center for Managing Non-Communicable Diseases of Ministry of Health and Medical Education, for analyzing the current situation of the country.One of the main ways for approaching the goals of Vision 2020 program is to develop the national documents for preventing blindness. According to the report of WHO, most East Mediterranean Region countries have developed their national plans.
The evidence shows that regarding the appropriate ratio of ophthalmologists to the population size[1], and also the acceptable coverage of eye surgeries by insurance companies in Iran, the main reason of the high prevalence of blindness and low vision in the country can be lack of an appropriate plan for delivering medical services, as well as the limited knowledge on the method of extending and maintaining health services.
By establishing the stewardship system, Iranians’ vision health can be improved and responsibilities of all extra and intrasectoral units on preventing blindness and improving vision health status can be determined. With start of delivering the comprehensive services on vision health, prevalence of blindness among children and adults can be reduced, and also an appropriate model can be provided for east Mediterranean region countries.
Regarding the PHC system of Iran, the first step for improving the vision health is empowerment of the community health workers (Behvarzes) for collaborating in screening and prevention blindness and low vision programs. Actions like educating general practitioners on the necessities of ophthalmology, recruiting at least one optometrist for each fifty thousand people at the first level of services and also providing at least one specialized center of eye service in each province,can cover the referred cases.
According to the results of this study and with considering obligations of all life stages, the intervention priorities for Iranian population are as follows:
Children (under ten years old): screening all of the population at birth (for congenital cataract, preterm retinopathy, and congenital glaucoma), vision examination at 3-5 years old, and examining strabismus by optometrist;
Adolescents (ten to eighteen years old): caring for refractive errors;
Young adults (eighteen to thirty years old): caring for diabetic retinopathy;
Adults (thirty to sixty-five years old): caring for glaucoma,cataract and diabetes;
Elderly (over sixty- five years old): caring for presbyopia and cataract;
Ophthalmologic emergencies at all ages.
Based on Table 3, the most important research priority in the field of eye health is continuous observation of the indicators.The institution of “Prevent Blindness America” believes the keys of its success are creating the national system of data gathering, national association of chronic disease, public education, behavioral risk factors surveillance, developing methods for integrating eye and vision surveillance in the public health system[17].
The three interventions suggested in this study for managing this issue are required a national committee for preventing blindness with participation of all stakeholders, implementing the national vision survey, preparation of the primary level health centers including employment and education of community health workers (Behvarzes), optometrists and general practitioners, fair distribution of specialized human resources and establishing at least one specialized center in each province for referring patients from the primary levels.
Limitation As a limitation, participation of all stakeholders in the planning phase was impossible. This can of course be removed by forming the national committee of preventing blindness at the start of the program. Another limitation was lack of enough information about Iranian’s vision health situation. In other words, there is not still any national survey and or a system of recording vision data in the country. This can make the targeting a difficult task. For removing this difficulty, it was suggested that the first year of the program to be devoted to implementing a national survey and creating a system for recording vision health data, so that a base year data can be accessed. In the other word, the most important research priority in the field of eye health is to establish a surveillance system for the needed indicators.
Recommendation It is suggested that the research priorities be determined by emphasizing on the information requirements of the PHC system. It can be done through a national work distribution among the research centers and scientific societies,in order to develop a surveillance system on the indicators of eye health.
Also, for operationalizing strategies indicated in this paper,obtaining an authoritative credit by the high council of health and food security is mandatory. In addition, an inter-sectoral cooperation agreement for preventing the avoidable blindness must be signed and monitored by all stakeholders.
ACKNOWLEDGEMENTS
Authors would like to thank the kind helps of Dr. Koorosh E’temad in implementing this study.
Foundation: Supported by Center of Managing Noncommunicable Diseases of Iran’s MOHME.
Conflicts of Interest: Damari B, None; Mahdavi A, None;Hajian M, None.
REFERENCES
1 Khanna RC, Marmamula S, Rao GN. International Vision Care: Issues and Approaches. Annu Rev Vis Sci 2017;3:53-68.
2 Ackland P. The accomplishments of the global initiative VISION 2020:The Right to Sight and the focus for the next 8 years of the campaign.Indian J Ophthalmol 2012;60(5):380-386.
3 Hogg K, Thetford C, Wheeler SL, York S, Moxon R, Robinson J. Habilitation provision for children and young people with vision impairment in the United Kingdom: a lack of clarity leading to inconsistencies. Br J Vis Impair 2017;35(1):44-54.
4 Bittle MJ. A new vision and leadership challenge: implementing the Affordable Care Act to improve the organization and delivery of health care services. J Public Health Manag Pract 2015;21(1):59-61.
5 Pararajasegaram R. VISION 2020-the right to sight: from strategies to action. Am J Ophthalmol 1999;128(3):359-360.
6 Sommer A, Taylor HR, Ravilla TD, West S, Lietman TM, Keenan JD,Chiang MF, Robin AL, Mills RP, Council of the American Ophthalmological Society. Challenges of ophthalmic care in the developing world. JAMA Ophthalmol 2014;132(5):640-644.
7 Sasongko MB, Widyaputri F, Agni AN, Wardhana FS, Kotha S, Gupta P, Widayanti TW, Haryanto S, Widyaningrum R, Wong TY, Kawasaki R,Wang JJ. Prevalence of diabetic retinopathy and blindness in indonesian adults with type 2 diabetes. Am J Ophthalmol 2017;181:79-87.
8 Crisp N, Chen L. Global supply of health professionals. N Engl J Med 2014;370(23):2247-2248.
9 Rajavi Z, Katibeh M, Ziaei H, Fardesmaeilpour N, Sehat M, Ahmadieh H, Javadi MA. Rapid assessment of avoidable blindness in Iran.Ophthalmology 2011;118(9):1812-1818.
10 Leasher JL, Lansingh V, Flaxman SR, Jonas JB, Keeffe J, Naidoo K,Pesudovs K, Price H, Silva JC, White RA, Wong TY, Resnikoff S, Taylor HR, Bourne RR, Vision Loss Expert Group of the Global Burden of Disease Study. Prevalence and causes of vision loss in Latin America and the Caribbean: 1990-2010. Br J Ophthalmol 2014;98(5):619-628.
11 Katibeh M, Blanchet K, Akbarian S, Hosseini S, Ahmadieh H, Burton MJ. Planning eye health services in Varamin district, Iran: a crosssectional study. BMC Health Serv Res 2015;15(1):140.
12 Naderian G, Iranpour R, Mohammadizadeh M, Najafabadi FF, Badiei Z, Naseri F, Naderian M, Sajadi V. The frequency of retinopathy of prematurity in premature infants referred to an ophthalmology clinic in Isfahan. Journal of Isfahan Medical School 2011;29(128).
13 Katibeh M, Eskandari A, Yaseri M, Hosseini S, Ziaei H. The gender issue in congenital and developmental cataract surgery. J Ophthalmic Vis Res 2013;8(4):308-313.
14 Javadi MA, Katibeh M, Rafati N, Dehghan MH, Zayeri F, Yaseri M, Sehat M, Ahmadieh H. Prevalence of diabetic retinopathy in Tehran province: a population-based study. BMC Ophthalmology 2009;9:12.
15 Rajavi Z, Moghadasifar H, Feizi M, Haftabadi N, Hadavand R,Yaseri M, Sheibani K, Norouzi G. Macular thickness and amblyopia. J Ophthalmic Vis Res 2014;9(4):478-483.
16 Hashemi H, Yekta A, Jafarzadehpur E, Nirouzad F, Ostadimoghaddam H, Eshrati B, Mohazzab-Torabi S, Khabazkhoob M. The prevalence of amblyopia in 7-year-old schoolchildren in Iran. Strabismus 2014;22(4):152-157.
17 Ojaghi H, Moghaddar R, Ahari SS, Bahadoram M, Amani F.Amblyopia prevention screening program in Northwest Iran (Ardabil). Int J Prev Med 2016;7.
18 Hashemi H, Yekta A, Jafarzadehpur E, Ostadimoghaddam H, Eshrati B, Mohazzab-Torabi S, Khabazkhoob M, Soroush S. The prevalence of strabismus in 7-year-old schoolchildren in iran. Strabismus 2015;23(1):1-7.
19 Hashemi H. Validity of uncorrected visual acuity measured in vision screening programs for detecting refractive errors. Iran J Ophthalmol 2014;26(3):121-128.
20 Shadpour K. Health sector reform in Islamic Republic of Iran. Hakim Research Journal 2006;9(3):1-18.
21 Movahedi M, Hajarizadeh B, Rahimi A, Arshinchi M, Amirhosseini K, Motlagh M. Trend and geographical inequality pattern of main health indicators in rural population of Iran. Hakim Research Journal 2008;10(4):1-10.
22 Pakravan M, Yazdani S, Shahabi C, Yaseri M. Superior versus inferior Ahmed glaucoma valve implantation. Ophthalmology 2009;116(2):208-213.
23 Shari fi-Rad J, Fallah F. Trachoma prevalence in rural areas of eastern Iran. New Microbes New Infect 2016;11:82-83.
24 Azizi-Soleiman F, Heidari-Beni M, Ambler G, Omar R, Amini M,Hosseini SM. Iranian risk model as a predictive tool for retinopathy in patients with type 2 diabetes. Can J Diabetes 2015;39(5):358-363.
25 Mohammadi SF, Saeedi-Anari G, AshrafiE, Mohammadi SM,Farzadfar F, Lashay A, Hashemi H. Prevalence and major causes of visual impairment in Iranian adults: a systematic review. Middle East Afr J Ophthalmol 2017;24(3):148-155.
26 Hashemi H, Kashi AH, Fotouhi A, Mohammad K. Distribution of intraocular pressure in healthy Iranian individuals: the Tehran Eye Study.Br J Ophthalmol 2005;89(6):652-657.
27 Hashemi H, Hatef E, Fotouhi A, Feizzadeh A, Mohammad K. The prevalence of lens opacities in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol 2009;16(3):187-192.
28 Fotouhi A, Khabazkhoob M, Hashemi H, Mohammad K. Sensitivity and specificity of visual screening tests in Dezful Schoolchildren, 2004.Iranian J Epidemiol 2007;3(1):11-17.
29 Hashemi H, Khabazkhoob M, Jafarzadehpur E, Yekta AA, Emamian MH, Shariati M, Fotouhi A. High prevalence of myopia in an adult population, Shahroud, Iran. Optom Vis Sci 2012;89(7):993-999.
30 Hashemi H, Yekta A, Nojomi M, Mohazzab-Torabi S, Behnia B,Khabazkhoob M. Excimer laser refractive surgery rate in Iran: 2010-2014.J Curr Ophthalmol 2018;30(4):311-314.
31 Soori H, Ali JM, Nasrin R. Prevalence and causes of low vision and blindness in Tehran Province, Iran. J Pak Med Assoc 2011;61(6):544-549.
32 Solebo AL, Teoh L, Rahi J. Epidemiology of blindness in children.Arch Dis Child 2017;102(9):853-857.
33 Katibeh M, Pakravan M, Yaseri M, Pakbin M, Soleimanizad R.Prevalence and causes of visual impairment and blindness in central iran;The Yazd Eye Study. J Ophthalmic Vis Res 2015;10(3):279-285.
34 Shahriari HA, Izadi S, Rouhani MR, Ghasemzadeh F, Maleki AR.Prevalence and causes of visual impairment and blindness in Sistanva-Baluchestan Province, Iran: Zahedan Eye Study. Br J Ophthalmol 2007;91(5):579-584.
35 Katibeh M, Ziaei H, Panah E, Moein HR, Hosseini S, Kalantarion M, Eskandari A, Yaseri M. Knowledge and awareness of age related eye diseases: a population-based survey. J Ophthalmic Vis Res 2014;9(2):223-231.
36 Hashemi H, Kashi AH, Fotouhi A, Mohammad K. Distribution of intraocular pressure in healthy Iranian individuals: the Tehran Eye Study.Br J Ophthalmol 2005;89(6):652-657.
37 Hashemi H, Fotouhi A, Mohammad K. The Tehran Eye Study: research design and eye examination protocol. BMC Ophthalmol 2003;3:8.
38 Dehghan A, Kianersi F, Moazam E, Ghanbari H. Causes and anatomical site of blindness and severe visual loss in Isfahan, Islamic Republic of Iran. Eastern Mediterranean Health Journal 2010;16(2):228-232.
39 Bressler NM, Varma R, Doan QV, Gleeson M, Danese M, Bower JK,Selvin E, Dolan C, Fine J, Colman S, Turpcu A. Underuse of the health care system by persons with diabetes mellitus and diabetic macular edema in the United States. JAMA Ophthalmology 2014;132(2):168-173.
40 Murray CJ1, Atkinson C, Bhalla K, et al. The state of US health, 1990-2010:burden of diseases, injuries, and risk factors. JAMA 2013;310(6):591-606.
41 Sharifzadeh M, Rahmanikhah E, Nakhaee N. Pattern of pediatric eye injuries in Tehran, Iran. Int Ophthalmol 2013;33(3):255-259.
42 Andriamanjato H, Mathenge W, Kalua K, Courtright P, Lewallen S.Task shifting in primary eye care: how sensitive and specific are common signs and symptoms to predict conditions requiring referral to specialist eye personnel? Hum Resour Health 2014;12(Suppl 1):S3.
Citation: Damari B, Mahdavi A, Hajian M. How to improve Iranians’vision health: on the national policy of preventing Iranians’ blindness.Int J Ophthalmol 2019;12(1):114-122
DOl:10.18240/ijo.2019.01.18
● KEYWORDS: vision health; policy document; primary health care
Received: 2018-2-12 Accepted: 2018-11-27
Correspondence to: Maryam Hajian. Minimally Invasive Surgery Research Center, Hazrat-e-Rasool Hospital, Shahid Mansouri Ave., Niyayesh St. Sattarkhan St., No.98, Tehran 1445613113, Iran. drmhajian@gmail.com