
・Review
Article・
Potential
of video games for the promotion of neuroadaptation to multifocal intraocular
lenses: a narrative review
María Begoña Coco-Martin1,2,
Pedro L. Valenzuela3, Miguel J. Maldonado-López2,
Alejandro Santos-Lozano4, Ainhoa Molina-Martín5, David P
Piñero5,6
1Research
Unit, Hospital Clínico Universitario de Valladolid. ICSCYL, Valladolid 47003,
Spain
2Grupo de
Cirugía Refractiva y Rehabilitación Visual. Instituto Universitario de
Oftalmobiología Aplicada (IOBA), Universidad de Valladolid, Valladolid 47011,
Spain
3Physiology
Unit, Systems Biology Department, University of Alcalá, Madrid 28801, Spain
4Grupo de
Investigación i+Health, Departamento de Ciencias de la Salud, Universidad
Europea Miguel de Cervantes, Valladolid 47012, Spain
5Department
of Optics, Pharmacology and Anatomy, University of Alicante, Alicante 03690,
Spain
6Department
of Ophthalmology (IMQO-Oftalmar), Vithas Medimar International Hospital,
Alicante 03016, Spain
Correspondence
to: David P. Piñero. Department of Optics, Pharmacology and
Anatomy, University of Alicante, Crta San Vicente del Raspeig s/n, 03690 San
Vicente del Raspeig, Alicante 03690, Spain. david.pinyero@ua.es
Received:
Abstract
Multifocal intraocular lenses (IOLs) are currently
usually implanted for the treatment of cataracts because they have been proved
to be superior to monofocal IOLs with respect to spectacle independence. In
turn, they are associated with a higher prevalence of dysphotopsia symptoms
that is one of the most common causes of patient dissatisfaction.
Neuroadaptation seems to play a major role in the optimal adaptation to
multifocal IOLs. In this context, the development of strategies that facilitate
the neuroadaptation process to multifocality might be an effective strategy to
reduce patients’ dissatisfaction. Video games have been proved to be effective
for the improvement of visual acuity and for the promotion of neuroplasticity
in elderly subjects and other populations with cortical-related visual
impairment. This narrative review highlights the physiological potential of
video games as a perceptual strategy to improve visual acuity and promote
neuroplasticity in patients using multifocal IOLs, although research is still
needed to confirm these benefits in this specific population, with only one
comparative study to this date providing evidence of them.
KEYWORDS: multifocal
intraocular lens; dysphotopsia; photic phenomena; halos; video games;
neuroadaptation; neuroplasticity
DOI:10.18240/ijo.2019.11.18
Citation: Coco-Martín
MB, Valenzuela PL, Maldonado-López MJ, Santos-Lozano A, Molina-Martín A, Piñero
DP. Potential of video games for the promotion of neuroadaptation to multifocal
intraocular lenses: a narrative review. Int J Ophthalmol
2019;12(11):1782-1787
INTRODUCTION
Societies are progressively aging,
which comes accompanied by an increased prevalence of age-related diseases[1]. Cataracts, that is,
the degeneration and subsequent opacity of crystalline lens, are one of these
diseases. In fact, they are among the leading causes of visual impairment,
especially in developing countries[2-3].
Cataract surgery techniques have
progressively improved, with around 90% of patients presenting optimal vision
acuity afterwards[4].
The standard intraocular lenses (IOLs) traditionally implanted (monofocal IOLs)
during cataract surgery have fixed refractive power and focal length, and
consequently most patients using these IOLs need glasses to improve their
vision at certain distances. In turn, multifocal IOLs offer full refractive
correction at all distances, and are therefore superior to monofocal IOLs with
respect to spectacle independence[5]. However, multifocal IOLs are associated with a higher
prevalence of visual disturbances (e.g., glare and haloes)[5], being low visual
acuity and specially dysphotopsia symptoms the main causes of dissatisfaction
in patients using these lenses[6-7].
The causes of the abovementioned
multifocal-related visual problems remain unclear. Parameters such as visual
acuity and other causes of impaired vision such as dry eye or retinal disease
seem not to be related to the incidence of dysphotopsic symptoms and the
associated dissatisfaction[6,8]. In turn, it has
been recently suggested that the activation of certain brain areas might play a
role in the adaptation to multifocal IOLs. There is an association between
multifocal IOL users’ difficulties and the activation of cortical areas
dedicated to attention (i.e. frontoparietal circuits), learning and
cognitive control (i.e. cingulate), and task goals (i.e. caudate)[8]. Indeed, improving
visual attention and procedural learning networks seems to be an essential part
of the initial stages of neuroadaptation to multifocal IOLs, as these neural
changes are associated with improvements in symptoms, visual acuity and
contrast sensitivity independently of optical factors[9].
In this context, the development of
strategies that facilitate the neuroadaptation process to multifocal IOLs might
be an effective approach to reduce patients’ dissatisfaction. The aim of this
narrative review was to summarize the evidence on the potential effectiveness
of video games for the promotion of neuroadaptation in the general population
as well as in individuals with vision impairment, as well as to describe the
characteristics of those video games that have shown beneficial effects. For
this purpose, we performed a non-systematic review in PubMed using the terms
“video games” or “computerized cognitive training” and terms such as brain
plasticity, neuroplasticity, neuroadaptation, cognition, visual acuity, vision,
visual impairment, cataract or amblyopia. Reference lists of relevant articles
and reviews were also examined to find additional publications on the topic.
VIDEO GAMES, A POSSIBLE SOLUTION
The Role of Videogames in
Neuroplasticity and Vision In this context, the development of
strategies that facilitate the neuroadaptation process to multifocal IOLs might
be an effective approach to reduce patients’ dissatisfaction. Video games have
been proved to promote brain plasticity. For instance, increases in gray matter
in areas crucial for spatial navigation, strategic planning, working memory and
motor performance (i.e., right hippocampal formation, right dorsolateral
prefrontal cortex and bilateral cerebellum) have been observed in young
subjects after two months of video game playing[10]. Similarly, other authors
reported an enhanced functional connectivity and grey matter volume in insular
sub-regions and between the attentional and sensorimotor networks in young
video game players[11].
Gaming can promote brain adaptations and improve functional connectivity even
at advanced age[12].
It has proven to attenuate age-related deficits in neural signatures of
cognitive control-reflected by enhanced midline frontal theta power and frontal
posterior theta coherence measured by means of electroencephalography-as well
as to improve sustained attention and working memory in older adults[13]. Moreover,
increases in neural activity (anterior P
Owing to the effects that these
‘therapies’ elicit in a variety of brain functions such as attention, cognitive
control and visuospatial skills[15], gaming and computerized strategies provide several
benefits in cognition and vision in elderly subjects[16-20]. Moreover, not only they can improve vision in healthy
individuals but also in clinical conditions, such as amblyopia[21]. Amblyopia is a
developmental abnormality characterized by an alteration in the visual cortex
that results in vision impairment (i.e., low visual acuity and contrast
sensitivity, and perception of crowding effect and suppression). The
traditional treatment for childhood amblyopia was occlusion therapy (i.e.,
patching the non-amblyopic eye), but more recent evidence demonstrated that the
inclusion of perceptual strategies such as playing video games with the
amblyopic eye can result in a more rapid improvement[22]. Indeed, it was traditionally
believed that amblyopia was irreversible beyond the sensitive period of brain
development during childhood. However, recent studies demonstrate that
perceptual training strategies can also enhance visual plasticity and improve
visual acuity and contrast sensitivity in adults with amblyopia[23-24].
Characteristics of Potentially
Effective Video Games for the Promotion of Neuroadaptation Different types of video games can
improve vision and cognitive function. Action video games, ones of the most
popular among young subjects, are probably the most effective for this purpose,
having proven to promote brain plasticity and enhance different variables such
as speed of processing, perception, attention or cognition[25-27]. However, most action video games share some
characteristics (are too fast, intense, unpredictable and sometimes even
violent) that make them unsuitable for older adults, the population that most
commonly suffer from cataracts. Indeed, this type of video games has been
reported as less interesting -inducing therefore a lower compliance- than
non-action video games in elderly adults[28-31], being intellectually stimulating games (e.g., puzzle,
simulation and strategy ones) the most appealing[28,32].
In this sense, non-action gaming
strategies that include cognitive training for the improvement of mental
abilities (the so called ‘brain training’ games), such as Nintendo game Brain
Age or the commercial games Lumosity (https://www.lumosity.com), Cogmed
(https://www.cogmed.com) or Fit Brains (http://www.fitbrains.com), which are
also available as smartphone applications, have shown promising results in
elderly subjects. This type of games has been reported to improve executive
function, processing speed, attention and visual recognition memory, and
working memory in this population[14,33-37], being the
benefits greater than those provided by other common games such as the falling
blocks (Tetris)[37].
Other authors observed a reduction of distraction and an increase of alertness
in older adults after 20 one-hour game training sessions compared to a control
group[38].
Moreover, improvements in inhibition and inductive reasoning have also been
reported in these individuals after this type of training when compared to a
control group that watched a documentary[39]. Some benefits can also be
obtained with driving simulation games, which have been reported to improve
multi-task performance, cognitive control, enhanced sustained attention and
working memory in older adults[13].
In summary, non-action video games
such as simulation and especially cognitive training ones appear as a promising
strategy for the improvement of vision in elderly subjects. However, as
abovementioned, the impaired vision of individuals with multifocal IOLs seem to
be largely related to a new and non-physiological focusing properties of the
retinal image formation that need development of novel suppression and
filtering strategies in the brain cortex, and consequently analyzing the gaming
strategies and cognitive stimuli that have previously demonstrated to be
effective in visual impairments related to cortical alteration, such as amblyopia,
could be especially useful for the optimal design of video games in this
population.
Perceptual training, which can be
conducted through playing video games, improves visual acuity in amblyopia,
reducing spatial distortion (internal neural noise) and increasing sampling
efficiency (the ability to extract stimulus information)[40]. Playing video games using only
the amblyopic eye (i.e., monocular training) has proven to enhance
visual and positional acuity, spatial attention and stereopsis in adults
through these neural adaptations[24]. However, a binocular alternative approach known as
dichoptic training has also been recently proposed. During this intervention,
high and low contrast stimuli are presented to the amblyopic and fellow eye,
respectively, in order to balance the input from both and enable binocular
integration. This strategy has also been reported to improve contrast
sensitivity and visual acuity in adults with amblyopia[41-42], and seems to be more effective for the improvement of
several visual functions than other strategies such as watching movies with a
patch on the non-amblyopic eye[43] or monocular training[44].
Thus, dichoptic training providing
different contrast stimuli for the operated and the fellow eye might be a
potentially effective strategy for the promotion of neuroadaptation to
multifocal IOLs, and consequently for the enhancement of visual acuity. For
example, games in which subjects drive a vehicle and some objects are just seen
with the ‘bad’ eye have been proved to be beneficial in amblyopia[45]. Similarly, the
Tetris game with some blocks being presented to both eyes but others just to
the amblyopic or the fellow eye at high and low contrast, respectively, is also
an alternative strategy for the improvement of vision[41,46].
Therapies including perceptual
learning signals have also shown remarkable results in subjects with myopia and
amblyopia[23,44,47], and could provide benefits in
patients with multifocal IOLs. In these games, subjects usually have to take
decisions (e.g., decide which button to click) depending on the Gabor
patch presented, with Gabor stimuli varying in number, spatial arrangement,
global and local orientation, target-flankers separation, exposure time or
contrast and spatial frequency. Moreover, the combination of dichoptic training
with perceptual learning might maximize the benefits[43-44]. Following the study of Vedamurthy et al[43] who demonstrated
that this strategy is effective for the improvement of visual acuity in
amblyopic adults, a discrimination perceptual learning task (e.g.,
Gabbor patch) can be presented to the operated eye during the game so that the
subject rapidly performs an action (e.g., clicking a button or not)
depending on its orientation.
Previous Experiences of Visual
Training in Eyes Implanted with Multifocal IOLs The scientific evidence to this date
of the use of visual training to improve the results of eyes undergoing
cataract surgery with implantation of multifocal IOLs is scarce[48-49]. Kaymak et al[48] evaluated the
effect of computer-based visual training in only one eye (with the fellow eye
occluded) of patients undergoing bilateral cataract surgery with implantation
of multifocal IOLs (apodized diffractive and bifocal diffractive designs). The
untrained fellow eye served as control. The training was performed during a
6-week postoperative period and based on the concept of perceptual learning of
discrimination line orientations. The presentation of the stimuli was done at a
fixed distance of
CONCLUSIONS AND FUTURE PERSPECTIVES
The popularity of multifocal IOLs
implantation after cataract surgery is rapidly growing because they have proven
superior to monofocal IOLs with respect to spectacle independence. However,
they are associated with a higher prevalence of other complications such as low
visual acuity and visual complains (e.g., dysphotopsia symptoms).
Promoting neuroadaptation to
multifocal IOLs seems to play a major role in the presence of symptoms in
patients using these lenses, and video games appear as a promising strategy for
this purpose (Figure 1). As shown in this narrative review, some evidence
suggests that gaming strategies might be effective for the promotion of
neuroplasticity and for the improvement of vision in elderly subjects and in
populations with cortical-related visual impairments such as amblyopia. Games
including cognitive training stimuli seem to be the most effective for the
enhancement of neuroplasticity in elderly subjects, as well as the most
appealing to this population. These benefits might be applicable to patients
using multifocal IOLs, as demonstrated initially by a first comparative study.
The benefit in these eyes may be in terms of visual performance as well as in
terms of less perception of photic phenomena.
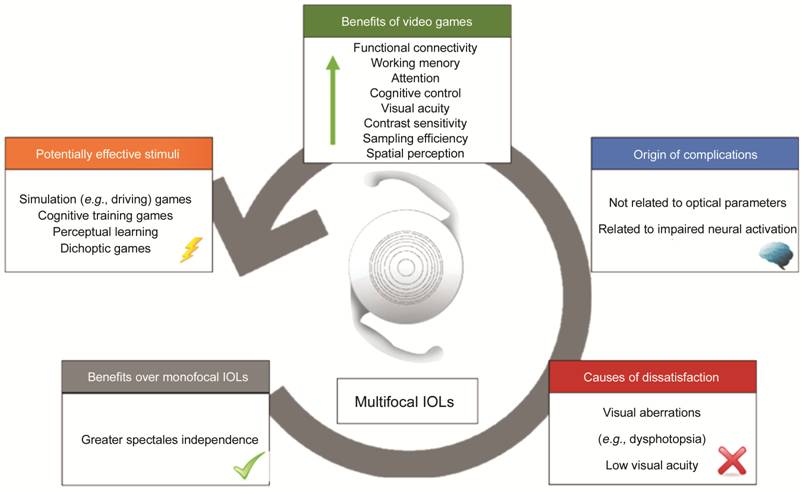
Figure 1 Graphic summary of
multifocal IOLs-related pros and cons, and of the potential benefits of video
games in these patients.
Notwithstanding, despite the
potential of video games for the promotion of neuroadaptation to multifocal
IOLs, research is still needed to confirm if they can effectively improve
visual acuity in these patients and decrease multifocal IOLs-related adverse
effects or reduce the postoperative time to reach satisfaction with vision
performance. Specifically, clinical trials are needed to provide more
consistent evidence of the use of this type of training with video games in
eyes implanted with multifocal IOLs.
ACKNOWLEDGEMENTS
This article
is part of the research performed in the context of the Project OPTiTRAIN,
(“Neuroentrenamiento visual en pacientes operados de cirugía de cataratas e
implantados con lente intraocular multifocal”, application number 106153).
Foundation: Coco-Martin
MB, Maldonado-López MJ, Molina-Martín A and Piñero DP are supported by CDTI
(Centro para el Desarrollo Tecnológico Industrial, Ministry of Economy and
Competitiveness of Spain) by means of the program PID (“Proyectos de
Investigación y Desarrollo”); The author Piñero DP has been also supported by
the Ministry of Economy, Industry and Competitiveness of Spain within the
program Ramón y Cajal (RYC-2016-20471); Valenzuela PL is supported by a
contract granted by University of Alcalá (FPI2016).
Conflicts of
Interest: Coco-Martín MB, None; Valenzuela PL, None;
Maldonado-López MJ, None; Santos-Lozano A, None; Molina-Martín A, None; Piñero
DP, None.
References