Th lymphocyte subsets in patients with Vogt-Koyanagi-Harada disease
Liang Liang1,2, Xiao-Yan Peng2, Hong Wang2
1The Fifirst Affiliated Hospital of Chongqing Medical University, Chongqing Key Laboratory of Ophthalmology, and Chongqing Eye Institute, Chongqing 400016, China
2Beijing Tongren Eye Center, Beijing Key Laboratory of Ophthalmology and Visual Science, Beijing Tongren Hospital,Capital Medical University, Beijing 100730, China
Abstract● AlM: To assess helper T (Th) lymphocyte subset balance in patients with Vogt-Koyanagi-Harada (VKH) disease.● METHODS: Sixty-eight active VKH patients and seventytwo inactive VKH patients were included in this study. One hundred healthy individuals served as controls. Peripheral blood was obtained from VKH patients and healthy controls.Th lymphocyte subsets were analyzed by flow cytometry.Plasma concentration of interleukin (lL)-17, lL-10, transforming growth factor (TGF)-β, lL-23 and lL-6 was examined by enzyme-linked immunosorbent assay (ELlSA).● RESULTS: VKH patients with active uveitis had significantly higher percentages of both Th1 and Th17 cells and lower percentages of regulatory T (Treg) cells as compared with inactive VKH patients and healthy controls. Th1/Th2 and Th17/Treg ratios were also significantly elevated in active VKH patients. The percentages of Th1, Th17 and Treg cells and the Th1/Th2, Th17/Treg ratio did not differ between inactive VKH patients and healthy controls. There was no difference concerning the percentage of Th2 cells among all the groups. VKH patients with active uveitis showed an elevated level of peripheral Th17 related cytokines levels (TGF-β, lL-6, lL-23, and lL-17) and a decreased level of Treg related cytokines (lL-10) compared with inactive VKH patients and healthy controls. lnactive VKH patients showed no differences in peripheral Th17 related cytokines (TGF-β, lL-6, lL-23, and lL-17) and Treg related cytokines (lL-10) levels compared with healthy controls.● CONCLUSlON: Th1 and Th17 cells are significantly increased and Treg cells significantly decreased in active VKH compared with inactive VKH or healthy controls.Therefore, Thlymphocyte subset analysis may serve as a disease biomarker for VKH.
INTRODUCTION
V ogt-Koyanagi-Harada (VKH) disease is one of the most common entities of uveitis in China and now is considered as an autoimmune disease. VKH disease is a kind of granulomatous panuveitis with systemic manifestations consisted of alopecia, vitiligo, poliosis and auditory/central nervous system symptoms[1-2]. Although a large number of researches have been performed, the exact mechanism of how VKH disease is onset and develop is now still not completely elucidated. Results of former investigations indicated that CD4+ helper T (Th) cells are involved in the occurrence of VKH disease[3-4]. Traditionally the CD4+ Th cells are considered to be subdivided into two subpopulations, Th1 and Th2, based on their cytokines production. Th1 cells synthesize interferon-γ(IFN-γ) and interleukin (IL)-2, however Th2 cells express IL-4,IL-10 and IL-5[5]. In classical immune theory the maintenance of a stable immune system depends on the balance of Th1 and Th2 cells[6-7]. Lately, CD4+ CD25+ regulatory T (Treg)cells and Th17 cells have been found as two entirely different subpopulations from Th1 and Th2 cells. Th17 cells express retinoic acid-related orphan receptor γt (RORγt), however Treg cells produce fork head/winged helix transcription factor(Foxp3). Th17 cells act critical roles during the process of allergic and autoimmunity responses mainly through synthesizing IL-17, while Treg cells' function is anti-inflammatory and keeping tolerance to self-antigens via producing IL-10 or by contact-dependent suppression[8]. The balance between Treg and Th17 together with Th1 and Th2 lymphocytes may thus play a key role in the process of autoimmune and inflammatory diseases[9]. The purposes of this research were investigating the Th lymphocyte subset balance in patients with VKH and assess whether it is associated with disease activity.
SUBJECTS AND METHODS
Ethical Approval This research was consented by the Tongren Hospital Science and Ethics Committee. All operations satisfied the dogmas of the Declaration of Helsinki.The informed consents were collected from each of the healthy controls and VKH patients. Ethical registration number:ChiCTR1800016183.
Subjects In total sixty-eight patients with active VKH and seventy-two patients with inactive VKH were included in this study. One hundred healthy individuals were enrolled as a control group. All the subjects were enrolled between March 2009 and May 2015 at the uveitis clinic of the Tongren Eye Center. VKH patients were diagnosed based on the diagnostic criteria made by an international committee[10].The patients with active VKH showed cells in the anterior chamber and vitreous, keratic precipitates, subretinal fluid,and new chorioretinal lesions. The extra ocular manifestations consisted of alopecia, tinnitus, dysacusis, poliosis, and vitiligo.The patients with inactive uveitis had no active intraocular Inflammation.
All active VKH patients did not have any prednisone or immunosuppressive agents before visiting our hospital. Blood specimens were taken from VKH patients with inactive uveitis after termination of all medications at least 3mo. The patients who have been included in active patients group would be counted in inactive group when their diseases turned into quiescence and stopped any medications for at least 3mo.The patients who suffered from recurrence of VKH would not be included in this study. None had autoimmune disease,inflammatory disease or collagen disease.
Cell Culture Of 20 mL peripheral blood was taken from every subject. Peripheral blood mononuclear cells (PBMCs) were separated via Ficoll-Hypaque density gradient centrifugation.Plasma was collected for measuring cytokines. PBMCs were directly transferred into tubes for Treg cells staining. To analyze Th1, Th2 and Th17 subsets, isolated PBMCs were seeded in 24-well plates at a concentration of 2×106 cells per well and cultured in medium 1640 (Gibco BRL, Gaithersburg,MD, USA) with brefeldin A (10 g/mL; Sigma Chemical, St.Louis, MO, USA), phorbol 12-myristate 13 acetate (25 ng/mL;Sigma Chemical, St. Louis, MO, USA), and ionomycin(1 g/mL; Sigma Chemical, St. Louis, MO, USA) at the condition of 37℃ and 5% CO2 for 4h and then aliquoted into tubes.
Flow Cytometry Analysis To analyze Th1, Th2 and Th17,PBMCs were cultured with anti-human CD4-phycoerythrin cyanin 5.1 (PC5; BD Biosciences, San Jose, CA, USA) at 4℃for 20min. To analyze Treg, PBMCs were cultured with antihuman CD4-PC5 and anti-human CD25-phycoerythrin (PE;Beckman Coulter, Fullerton, CA, USA). Then, the cells were stained with anti-human INF-γ- fluorescein isothiocyanate for Th1 measurement, anti-human IL-4-PE for Th2 measurement,anti-human IL-17-allophycocyanin (APC; R&D Systems,Minneapolis, MN, USA) for Th17 measurement and antihuman Foxp3-Alexa Flour 488 (BioLegend, San Diego, CA,USA) for Treg measurement. Detection was executed by a FACS cytometer (Beckman Coulter, Fullerton, CA, USA).Gate A was made in FSC INT/FSC PEAK picture after the adhesion cells were excluded. Then gate B was made in FSC/SSC picture after excluded the dead cells. Gate G which represented lymphocyte was made in gate B. Gate H which represented CD4+ T lymphocyte was made in gate G. Then the ratios of INF-γ+, IL-4+, IL-17+ and CD25/Foxp3+ cells were displayed respectively.
Enzyme-linked Immunosorbent Assay for Interleukin-17,Interleukin-23, Interleukin-6, Interleukin-10 and Transforming Growth Factor-β The levels of IL-6, IL-10,IL-23, IL-17 and transforming growth factor (TGF)-β were detected by enzyme-linked immunosorbent assay (ELISA)according to the manufacturer's instructions (IL-17 ELISA kits, from Biosource, Nivelles, Belgium; IL-6, IL-10, IL-23 and TGF-β ELISA kits, from R&D system, Minneapolis, MN,USA).
Statistical Analysis One way ANOVA test was used to analyze the data. P values less than 0.05 were considered to be statistically significant.
RESULTS
Clinical Characteristics of Healthy Controls and Vogt-Koyanagi-Harada Patients The active VKH patients enrolled in this study were consisted of 32 men and 36 women,with an average age of 36y. The inactive VKH patients were consisted of 35 men and 37 women, with an average age of 38y. Healthy controls included 48 men and 52 women, with an average age of 35.2y. Healthy controls and VKH patients showed no significant differences in gender and age (Table 1).
Circulating Th1, Th2, Treg and Th17 Frequencies and Th1/Th2, Th17/Treg Ratios in Vogt-Koyanagi-Harada Patients The active VKH patients had significantly higher percentages of Th1 and Th17 cells and a lower percentage of Treg cells in their circulation as compared with healthy controls. The ratios of Th1/Th2 and Th17/Treg were significantly elevated in active VKH patients as well. No differences in the percentages of Th2 cells could be tested between active VKH patients and healthy controls. The inactive VKH patients showed no differences in the percentages of Th1, Th2, Treg, Th17 cells and the ratios of Th1/Th2 or Th17/Treg as compared with the healthy controls.Compared with the inactive VKH patients, the active VKH patients had significantly higher percenta ges of Th17 and Th1 cells and lower percentages of Treg cells (Table 2). The ratios of Th1/Th2 and Th17/Treg were also significantly elevated in active VKH patients. No differences in the percentages of Th2cells could be detected between active VKH patients and the inactive VKH patients.
Table 1 Characteristics of the subjects mean±SD
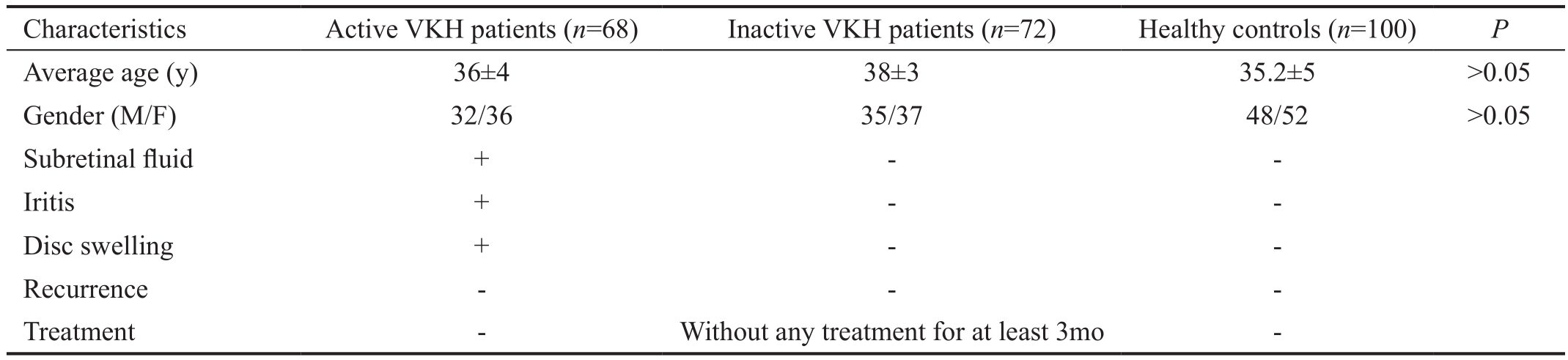
VKH: Vogt-Koyanagi-Harada.
 Average age (y) 36±4 38±3 35.2±5 >0.05 Gender (M/F) 32/36 35/37 48/52 >0.05 Subretinal fluid + - -Iritis + - -Disc swelling + - -Recurrence - - -Treatment - Without any treatment for at least 3mo -
Average age (y) 36±4 38±3 35.2±5 >0.05 Gender (M/F) 32/36 35/37 48/52 >0.05 Subretinal fluid + - -Iritis + - -Disc swelling + - -Recurrence - - -Treatment - Without any treatment for at least 3mo -
Table 2 Th lymphocyte subsets in patients with VKH disease mean±SD, pg/mL
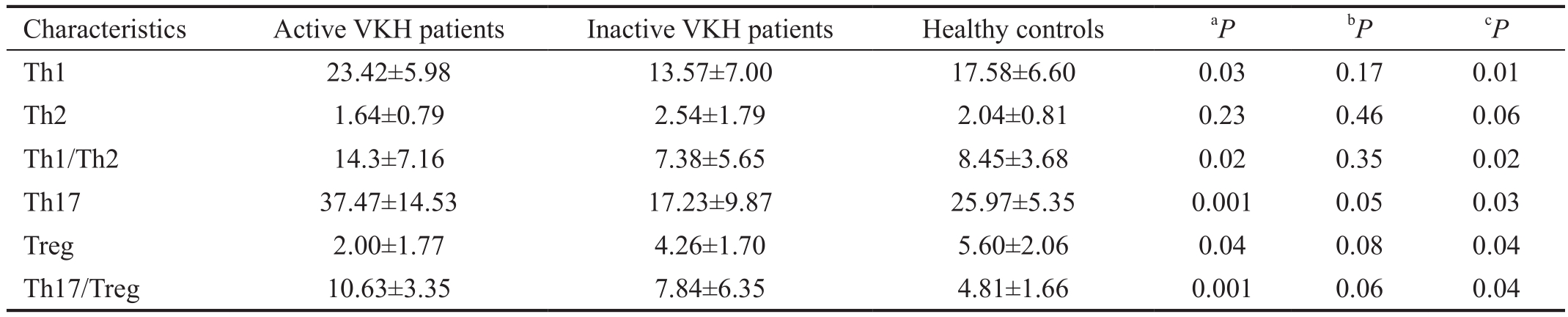
VKH: Vogt-Koyanagi-Harada.aHealthy controls vs active patients;bHealthy controls vs inactive patients;cActive patients vs inactive patients.
 Th1 23.42±5.98 13.57±7.00 17.58±6.60 0.03 0.17 0.01 Th2 1.64±0.79 2.54±1.79 2.04±0.81 0.23 0.46 0.06 Th1/Th2 14.3±7.16 7.38±5.65 8.45±3.68 0.02 0.35 0.02 Th17 37.47±14.53 17.23±9.87 25.97±5.35 0.001 0.05 0.03 Treg 2.00±1.77 4.26±1.70 5.60±2.06 0.04 0.08 0.04 Th17/Treg 10.63±3.35 7.84±6.35 4.81±1.66 0.001 0.06 0.04
Th1 23.42±5.98 13.57±7.00 17.58±6.60 0.03 0.17 0.01 Th2 1.64±0.79 2.54±1.79 2.04±0.81 0.23 0.46 0.06 Th1/Th2 14.3±7.16 7.38±5.65 8.45±3.68 0.02 0.35 0.02 Th17 37.47±14.53 17.23±9.87 25.97±5.35 0.001 0.05 0.03 Treg 2.00±1.77 4.26±1.70 5.60±2.06 0.04 0.08 0.04 Th17/Treg 10.63±3.35 7.84±6.35 4.81±1.66 0.001 0.06 0.04
Table 3 TGF-β, IL-6, IL-10, IL-23 and IL-17 in patients with VKH disease mean±SD, pg/mL

VKH: Vogt-Koyanagi-Harada.aHealthy controls vs active patients;bHealthy controls vs inactive patients;cActive patients vs inactive patients.
 IL-17 12.68±3.43 10.31±2.00 9.55±1.02 0.01 0.34 0.03 IL-23 11.67±9.52 7.84±2.58 6.71±0.76 0.06 0.26 0.04 IL-6 5.16±5.00 4.03±8.40 3.99±0.34 0.02 0.05 0.04 TGF-β 3890.14±2529.36 1825.46±1316.31 1721.94±1269.82 0.03 0.06 0.01 IL-10 7.00±6.85 21.96±7.65 22.04±7.36 0.04 0.08 0.01
IL-17 12.68±3.43 10.31±2.00 9.55±1.02 0.01 0.34 0.03 IL-23 11.67±9.52 7.84±2.58 6.71±0.76 0.06 0.26 0.04 IL-6 5.16±5.00 4.03±8.40 3.99±0.34 0.02 0.05 0.04 TGF-β 3890.14±2529.36 1825.46±1316.31 1721.94±1269.82 0.03 0.06 0.01 IL-10 7.00±6.85 21.96±7.65 22.04±7.36 0.04 0.08 0.01
Plasma Cytokine Levels in Vogt-Koyanagi-Harada Active VKH patients showed significant higher levels of cytokines related with Th17 (TGF-β, IL-6, IL-23, and IL-17) and an obvious lower level of cytokines related with Treg (IL-10) as compared with inactive VKH patients and healthy controls.Inactive VKH patients showed no differences in peripheral Th17 related cytokines (TGF-β, IL-6, IL-23, and IL-17) and Treg related cytokine (IL-10) plasma levels as compared with healthy controls. Compared with inactive VKH patients, the VKH patients with active uveitis had noticeably higher plasma levels of cytokines related with Th17 (IL-6, IL-17, IL-23, and TGF-β) and lower levels of cytokines related with Treg (IL-10;Table 3).
DISCUSSION
This study shows that disease activity in VKH disease is related with a significant increase in the circulating proinflammatory Th1 and Th17 lymphocyte subpopulations and a concomitant decrease in the Treg subset. Similar alterations were observed in the signature cytokines of these lymphocyte subsets indicating a role for an imbalanced systemic immune system in the development of VKH disease. Our study confirms and extends earlier findings from our group showing an increased production of IL-17 of CD4 positive T cells and PBMCs from active VKH patients treated with anti-CD28 and anti-CD3 antibodies[11]. We also reported that IFN-γ, IL-17 and RORγt were increased in active VKH patients and that cyclosporin A and corticosteroids could decrease these elevated cytokines levels which were related with the clinical relief of the uveitis[12]. It has been showed that cyclosporin A and dexamethasone could reduce Th1 and Th17 cells frequencies and decrease the IL-17 or IFN-γ release. All these results indicate that an increased response of Th17 and Th1 is related to active VKH disease and that corticosteroids and cyclosporin A may execute their immunosuppressive role by decreasing Th17 and Th1 cells.
Studies from various laboratories have now shown that the Th17 subset exerts a key role in the development of various autoimmune diseases by mainly producing IL-17[13-14]. It has been proved that IL-17 acts as a proinflammatory factor in vitro and vivo by inducing the expression of chemokines (such as monocyte chemotactic protein-1) and cytokines (such as TNF-α and IL-6)[15]. It has also been observed that the IL-17 level was increased in many autoimmune diseases such as multiple sclerosis[16], rheumatoid arthritis[17] and inflammatory bowel disease[18], indicating that IL-17 may act a critical role in the development of these diseases. Furthermore, in IL-17-/-mice collagen induced arthritis and experimental autoimmune encephalomyelitis, the animal models for rheumatoid arthritis and multiple sclerosis, respectively, could not be induced[19-20].Thus, there is a strong possibility that Th17 cells are involved in autoimmunity and that targeting these cells may provide an attractive option for immunotherapy of these diseases. It has also been proved that CD4+ CD25+ Foxp3+ Treg cells could effectively suppress the development of autoimmune disease[8]. In many autoimmune diseases, decreased number of Treg cells has been observed[21-24], and several autoimmune disorders have been shown to be relieved by adoptive transfer of purified Treg cells[25-28]. One study has demonstrated that in patients with active VKH Treg frequencies and functional properties were decreased[29]. Th17/Treg functional imbalance has also been found existed in atherosclerosis. In this study,we found that Treg cells frequencies were significantly lower in VKH patients with active uveitis as compared with healthy controls and inactive VKH patients. These findings confirm the hypothesis that Treg cells have a potential protective effect in the pathogenesis of VKH.
Treg cells perform their anti-inflammatory function mainly by expressing IL-10. In this study, the results showed that the level of IL-10 in plasma was decreased in active VKH, suggesting that IL-10 may exert a protective role in this disease.
A limitation of our study is that we studied only four subsets of Th lymphocyte. There are other subsets in Th lymphocyte such as Th9, Th22 and Tfh. Further investigations are needed to elucidate the changes of other subsets of Th lymphocyte. In summary, our data show a dysfunctional lymphocyte subset balance in patients with VKH and suggest that lymphocyte subset analysis might be used as a disease marker.
ACKNOWLEDGEMENTS
The authors thank Yang Wang and Bin-Bin Hou for their technical assistance and acknowledge the help of Professor Aize Kijlstra for editorial assistance.
Authors' contributions: Data collection, analysis and manuscript write up was performed primarily by the corresponding author, Hong Wang with the support of Liang Liang and Xiao-Yan Peng. Cytokine profile and flow cytometry analysis was supported by Liang Liang and was a major contributor to the manuscript. All authors have read and approved the final manuscript.
Foundations:Supported by National Natural Science Foundation of China (No.30772013); Basic Research Program of Chongqing (No.cstc2015jcyjA10112).
Conflicts of Interest:Liang L, None; Peng XY, None; Wang H, None.
REFERENCES
1 Burkholder BM. Vogt-Koyanagi-Harada disease. Curr Opin Ophthalmol 2015;26(6):506-511.
2 Sakata VM, da Silva FT, Hirata CE, de Carvalho JF, Yamamoto JH. Diagnosis and classification of Vogt-Koyanagi-Harada disease.Autoimmun Rev 2014;13(4-5):550-555.
3 Wu L, Wen H, Zhou Y, Yu H, Liu Y, Bai L, Kijlstra A, Yang P.Activation of the liver X receptor inhibits Th17 and Th1 responses in Behcet's disease and Vogt-Koyanagi-Harada disease. Curr Mol Med 2014;14(6):712-722.
4 Abad S, Wieers G, Colau D, Wildmann C, Delair E, Dhote R, Brezin AP,Kawakami Y, Coulie PG, van der Bruggen P. Absence of recognition of common melanocytic antigens by T cells isolated from the cerebrospinal fluid of a Vogt-Koyanagi-Harada patient. Mol Vis 2014;20:956-969.
5 Harrington LE, Mangan PR, Weaver CT. Expanding the effector CD4 T-cell repertoire: the Th17 lineage. Curr Opin Immunol 2006;18(3):349-356.
6 Li MO, Wan YY, Flavell RA. T cell-produced transforming growth factor-beta1 controls T cell tolerance and regulates Th1- and Th17-cell differentiation. Immunity 2007;26(5):579-591.
7 Thakker P, Leach MW, Kuang W, Benoit SE, Leonard JP, Marusic S. IL-23 is critical in the induction but not in the effector phase of experimental autoimmune encephalomyelitis. J Immunol 2007;178(4):2589-2598.
8 Sakaguchi S, Ono M, Setoguchi R, Yagi H, Hori S, Fehervari Z,Shimizu J, Takahashi T, Nomura T. Foxp3+ CD25+ CD4+ natural regulatory T cells in dominant self-tolerance and autoimmune disease.Immunol Rev 2006;212:8-27.
9 Homey B. After TH1/TH2 now comes Treg/TH17: significance of T helper cells in immune response organization. Hautarzt 2006;57(8):730-732.
10 Read RW, Holland GN, Rao NA, Tabbara KF, Ohno S, Arellanes-Garcia L, Pivetti-Pezzi P, Tessler HH, Usui M. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an international committee on nomenclature. Am J Ophthalmol 2001;131(5):647-652.
11 Chi W, Yang P, Li B, Wu C, Jin H, Zhu X, Chen L, Zhou H, Huang X, Kijlstra A. IL-23 promotes CD4+ T cells to produce IL-17 in Vogt-Koyanagi-Harada disease. J Allergy Clin Immunol 2007;119(5):1218-1224.
12 Liu X, Yang P, Lin X, Ren X, Zhou H, Huang X, Chi W, Kijlstra A,Chen L. Inhibitory effect of cyclosporin A and corticosteroids on the production of IFN-gamma and IL-17 by T cells in Vogt-Koyanagi-Harada syndrome. Clin Immunol 2009;131(2):333-342.
13 Knochelmann HM, Dwyer CJ, Bailey SR, Amaya SM, Elston DM,Mazza-McCrann JM, Paulos CM. When worlds collide: Th17 and Treg cells in cancer and autoimmunity. Cell Mol Immunol 2018;15(5):458-469.
14 Krohn S, Nies JF, Kapffer S, Schmidt T, Riedel JH, Kaffke A, Peters A, Borchers A, Steinmetz OM, Krebs CF, Turner JE, Brix SR, Paust HJ,Stahl RAK, Panzer U. IL-17C/IL-17 receptor E signaling in CD4(+) T cells promotes TH17 cell-driven glomerular inflammation. J Am Soc Nephrol 2018;29(4):1210-1222.
15 Kolls JK, Linden A. Interleukin-17 family members and Inflammation.Immunity 2004;21(4):467-476.
16 Mahmoud FM, ElSheshtawy NM, Zaki WK, Zamzam DM, Fahim NM. MicroRNA 26a expression in peripheral blood mononuclear cells and correlation with serum interleukin-17 in relapsing-remitting multiple sclerosis patients. Egypt J Immunol 2017;24(2):71-82.
17 Dhaouadi T, Chahbi M, Haouami Y, Sfar I, Abdelmoula L, Ben Abdallah T, Gorgi Y. IL-17A, IL-17RC polymorphisms and IL17 plasma levels in Tunisian patients with rheumatoid arthritis. PLoS One 2018;13(3):e0194883.
18 Wang Y, Mao Y, Zhang J, Shi G, Cheng L, Lin Y, Li Y, Zhang X,Zhang Y, Chen X, Deng J, Su X, Dai L, Yang Y, Zhang S, Yu D, Wei Y,Deng H. IL-35 recombinant protein reverses inflammatory bowel disease and psoriasis through regulation of inflammatory cytokines and immune cells. J Cell Mol Med 2018;22(2):1014-1025.
19 Nakae S, Nambu A, Sudo K, Iwakura Y. Suppression of immune induction of collagen-induced arthritis in IL-17-deficient mice. J Immunol 2003;171(11):6173-6177.
20 Komiyama Y, Nakae S, Matsuki T, Nambu A, Ishigame H,Kakuta S, Sudo K, Iwakura Y. IL-17 plays an important role in the development of experimental autoimmune encephalomyelitis. J Immunol 2006;177(1):566-573.
21 Owczarczyk-Saczonek A, Czerwinska J, Placek W. The role of regulatory T cells and anti-inflammatory cytokines in psoriasis. Acta Dermatovenerol Alp Pannonica Adriat 2018;27(1):17-23.
22 Ebrahimi M, Ganji A, Zahedi S, Nourbakhsh P, Ghasami K, Mosayebi G. Characterization of regulatory T-cells in multiple sclerosis patients treated with interferon beta-1a. CNS Neurol Disord Drug Targets 2018;17(2):113-118.
23 Li SL, Yu Y, Yang P, Wang H, Zhang C, Liu M, Zhang JX, Shen T, Wu C,Zhu QX. Trichloroethylene alters Th1/Th2/Th17/Treg paradigm in mice:a novel mechanism for chemically induced autoimmunity. Int J Toxicol 2018;37(2):155-163.
24 LaMothe RA, Kolte PN, Vo T, Ferrari JD, Gelsinger TC, Wong J, Chan VT, Ahmed S, Srinivasan A, Deitemeyer P, Maldonado RA, Kishimoto TK. Tolerogenic nanoparticles induce antigen-specific regulatory T cells and provide therapeutic efficacy and transferrable tolerance against experimental autoimmune encephalomyelitis. Front Immunol 2018;9:281.
25 Morgan ME, Flierman R, van Duivenvoorde LM, Witteveen HJ, van Ewijk W, van Laar JM, de Vries RR, Toes RE. Effective treatment of collagen-induced arthritis by adoptive transfer of CD25+ regulatory T cells. Arthritis Rheum 2005;52(7):2212-2221.
26 Denning TL, Kim G, Kronenberg M. Cutting edge: CD4+CD25+regulatory T cells impaired for intestinal homing can prevent colitis. J Immunol 2005;174(12):7487-7491.
27 Tang Q, Henriksen KJ, Bi M, Finger EB, Szot G, Ye J, Masteller EL,McDevitt H, Bonyhadi M, Bluestone JA. In vitro-expanded antigenspecific regulatory T cells suppress autoimmune diabetes. J Exp Med 2004;199(11):1455-1465.
28 Mekala DJ, Geiger TL. Immunotherapy of autoimmune encephalomyelitis with redirected CD4+CD25+ T lymphocytes. Blood 2005;105(5):2090-2092.
29 Chen L, Yang P, Zhou H, He H, Ren X, Chi W, Wang L, Kijlstra A.Diminished frequency and function of CD4+CD25high regulatory T cells associated with active uveitis in Vogt-Koyanagi-Harada syndrome. Invest Ophthalmol Vis Sci 2008;49(8):3475-3482.
Correspondence to: Hong Wang. Beijing Tongren Eye Center,Beijing Tongren Hospital, No.1 Dongjiaominxiang Road,Beijing 100730, China. wanghongyk@sina.com
Received: 2018-04-02 Accepted: 2018-06-07
● KEYWORDS:Vogt-Koyanagi-Harada disease; Th lymphocyte; Th17 cell; Treg cell; cytokines
DOl:10.18240/ijo.2019.02.04
Citation:Liang L, Peng XY, Wang H. Th lymphocyte subsets in patients with Vogt-Koyanagi-Harada disease. Int J Ophthalmol 2019;12(2):207-211