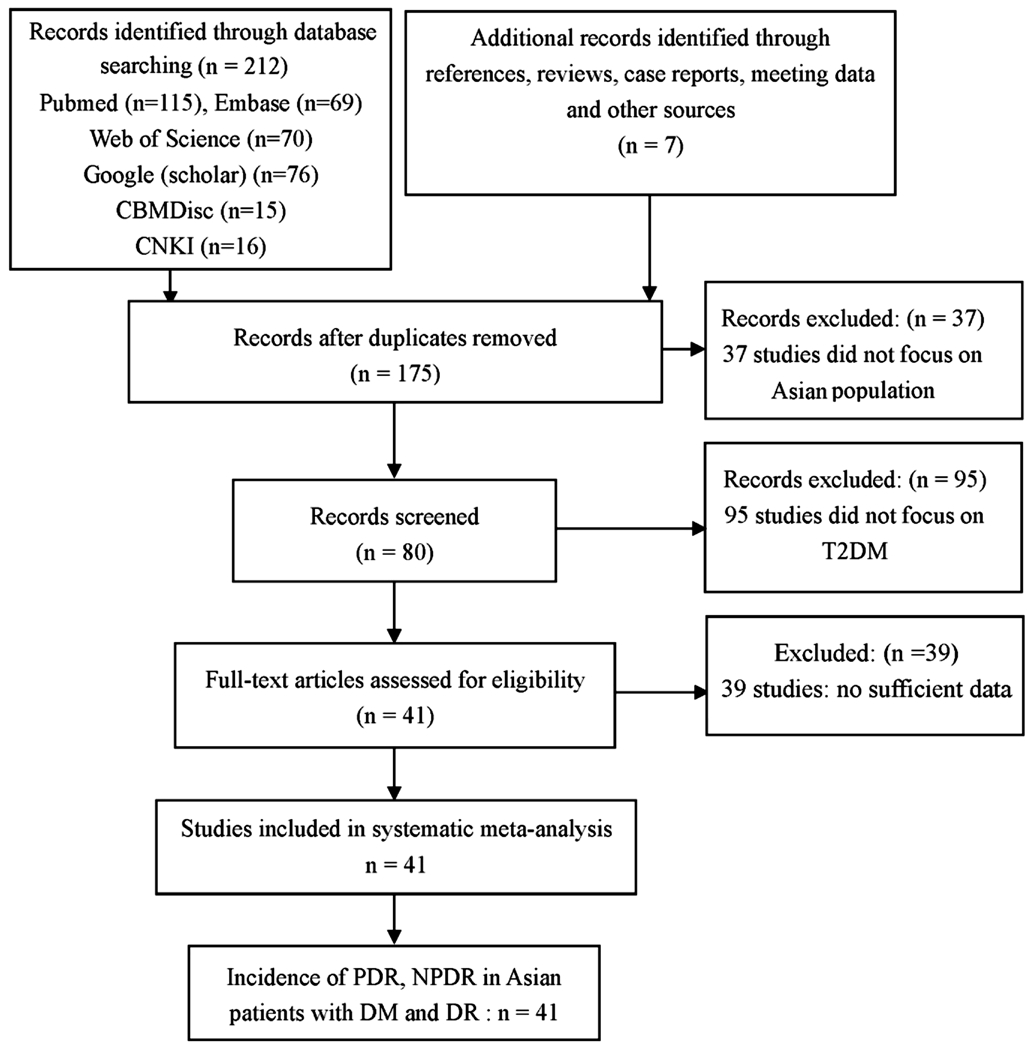
Figure 1 Flow chart showing the process of selection.
Type 2 diabetes mellitus (T2DM) is now considered as a growing world-wide health concern[1]. Nearly 180 million adults were reported to suffer from diabetes in 1980. The number of T2DM increased to 422 million in 2014[1], which is expected to be more than 552 million in 2030[2]. Several related complications have been observed in T2DM, such as diabetic nephropathy[3], diabetic cardiovascular diseases[4] and diabetic retinopathy (DR)[5]. Among these complications, DR is a common one and is classified as a microvascular damage disease, which includes two subtypes: nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy(PDR)[6]. DR is a leading cause of blindness in workingage adults with T2DM. According to statistics, once T2DM patients are diagnosed as DR, it will progress to vision threaten stage in approximately 11% patients every year, making DR a public health challenge[7].
It is believed that optimal screening strategies for DR in T2DM is necessary to public health due to its disastrous outcomes.Therefore, it is crucial to explore the prevalence of DR as well as PDR and NPDR in T2DM patients to provide further evidence for screening strategies. However, the prevalence of DR and PDR in different researches remains controversial. In Huang et al's[8] research, the prevalence of DR in Singaporean,Indian and Chinese populations was 36.88%, 36.47% and 30.30%, respectively, and the prevalence of PDR was 27.72%,25.82% and 26.57%, respectively, which was inconsistent with Thomas et al's[9] study, who reported that the prevalence of PDR in South Africa was 6.6%. In Stolk et al's[10] study,the prevalence of DR in Caucasian, Chinese and South Asian populations was 31.3%, 49.4% and 46.0% respectively, and the prevalence of PDR in Caucasian, Chinese and South Asian population was 1.2%, 3.5% and 1.7%, respectively.
Previous Meta-analyses have been performed to explore the prevalence of DR, PDR and NPDR in Iran and Chinese populations; however, these results were also con fl icting[11-12].Maroufizadeh et al[12] recruited thirty-one studies involving 23 729 patients with type 1 and 2 diabetes. Their results showed that the prevalence of DR, NPDR and PDR in Iranian diabetic patients were 41.9% (95%CI: 35.6-48.2),32.2% (95%CI: 28.7-35.8), and 13.2% (95%CI: 8.3-18.1),respectively. In Liu et al's[11] study, the prevalence of DR,NPDR and PDR in the pooled general population was 1.3%(95%CI: 0.5%-3.2%), 1.1% (95%CI: 0.6%-2.1%), and 0.1%(95%CI: 0.1%-0.3%), respectively, but was 23% (95%CI:17.8%-29.2%), 19.1% (95%CI: 13.6%-26.3%), and 2.8%(95%CI: 1.9%-4.2%) in the diabetic group. Due to this con fl icting result of Meta-analysis and the fact that no Metaanalysis and sub-analysis has been performed to detect this issue in other Asian countries, we performed this systematic review and Meta-analysis to investigate the pooled prevalence of DR, PDR and NPDR in Asian T2DM patients.
Literature Search A systematic online search was conducted to find out all the eligible studies that reported the prevalence of DR, NPDR and PDR in Asian populations. Databases including ‘PubMed', ‘EMBASE', ‘Web of Science', ‘Cochrane Library' and ‘China WeiPu Library' were searched. The following search terms were used to identify all the relevant studies: (‘prevalence' OR ‘incidence') AND (‘diabetic retinopathy' OR ‘nonproliferative diabetic retinopathy' OR‘proliferative diabetic retinopathy' OR ‘DR' OR ‘PDR' OR‘NPDR'). Then, studies were screened according to their study populations. There were no language and date restrictions in our searching procedure. The reference lists of the recruited studies, reviews or conference reports were also searched.Furthermore, the reviews and comments were also searched.All the analyses involved in our study were based on previous published studies, thus no ethical approval and patient consent are required.
Figure 1 Flow chart showing the process of selection.
Inclusion and Exclusion Criteria The inclusion criteria were as follows: 1) studies with prevalence estimates of DR, PDR and NPDR, including the numbers of DR, PDR, NPDR and T2DM; 2) study populations in Asian countries. The exclusion criteria were as follows: 1) intervention or treatment studies;2) no usable data reported; 3) duplicated studies. In addition,studies that reported the prevalence of DR, PDR and NPDR in T1DM were also excluded. The progress for study inclusion is shown in Figure 1.
Data ExtractionTwo authors extracted the general information and data in each study according to the inclusion and exclusion criteria, and a consensus was reached by discussion. If there was any disagreement, a third author would extract them, which was solved by consensus. Data were extracted using a standard form. The following data were collected: author, publish year, ethnicity, age, number of T2DM, DR, NPDR and PDR, and the total sample size.We also contacted the corresponding authors if there were incomplete data in recruited studies.
Quality AssessmentNewcastle Ottawa Quality Assessment Scale (NOQAS)[13] was used to assess the quality of all studies including non-randomized case controlled studies.
Data SynthesisEffect size (ES) with 95%CI was assessed to analyze the pooled prevalence of DR, PDR and NPDR in T2DM populations. The prevalence of PDR and NPDR in DR populations were also performed. Subgroup analysis according to the ethnicity of populations was also performed.The heterogeneity of included studies was examined by a Chi-squared-based Q statistical test and quantified by I2 metric value. If I2 value was more than 50% or P<0.10, ES was pooled by the random effect model; otherwise, the fixed effect model was used. Sensitivity analysis was performed to assess the impact of each study on the combined effect of the present Meta-analysis. Stata 12.0 software (StataCorp, College Station, TX, USA) was used, and a P<0.05 was considered as statistically significant.
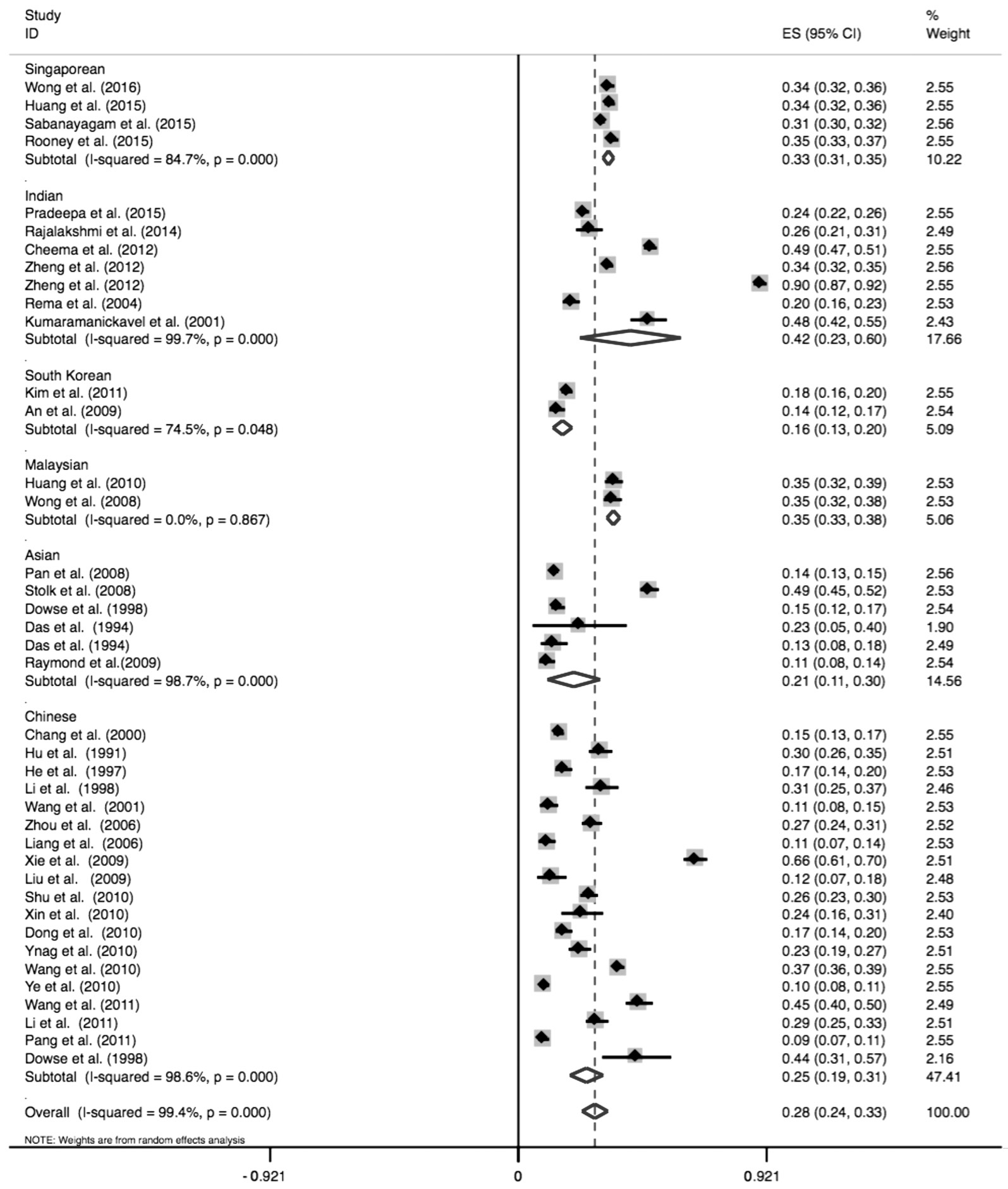
Figure 2 Forest plot of prevalence of DR in Singaporean, Indian, South Korean, Malaysian, Asian and Chinese populations.
Study Selection and CharacteristicsA total of 41 studies were finally included in our study (Figure 1). Of 6 studies were performed in Asian populations[14-19]; 4 studies were conducted in Singaporean group[8,20-23]; 7 studies were conducted in Indian group[23-28]; 2 studies were performed in South Korean group[29-30]; 2 studies were conducted in Malaysian populations[14,31] and 20 studies were performed in Chinese group[19,32-50]. And 10 studies reported the numbers of DR and DM[8,14-15,17,21-23,35,46], while 31 studies reported the numbers of DR, PDR, NPDR and DM[10,16,19,24-34,36-37,39-45,47-49,51-52]. The general characteristics of included studies were shown in Table 1.
Quality Assessment The quality assessments of studies are shown in Table 2, and we considered that the quality of each study was relatively high. In our study, 5 researches scored 9 points[7,19,24,30,43]; 27 studies scored 8 points[8,10,14,16-19,22-23,25-26,28,31-35,37,40-43,46,48-49]; 9 researches scored 7 points[15,17,28-29,36,38-39,45,51].
Meta-analysis Results Overall, the prevalence of DR in Asian T2DM patients was 28% (95%CI: 24%-33%). Subgroup analysis showed that the prevalence of DR in Singaporean,Indian, South Korean, Malaysian, Asian and Chinese populations was 33% (95%CI: 31%-35%), 42% (95%CI:23%-60%), 16% (95%CI: 13%-20%), 35% (95%CI: 33%-38%),21% (95%CI: 11%-30%), and 25% (95%CI: 19%-31%),respectively, as indicated in Table 3 and Figure 2.
In the overall Asian populations, the prevalence of PDR in DM patients was 6% (95%CI: 5%-7%). Our results also showed that the prevalence of PDR in Indian, South Korean,Malaysian, Asian and Chinese populations was 17% (95%CI:8%-26%), 3% (95%CI: 0-6%), 5% (95%CI: 3%-6%), 2%(95%CI: 0-4%) and 3% (95%CI: 2%-4%), respectively(Table 3).
Table 1 The general characteristics of included studies
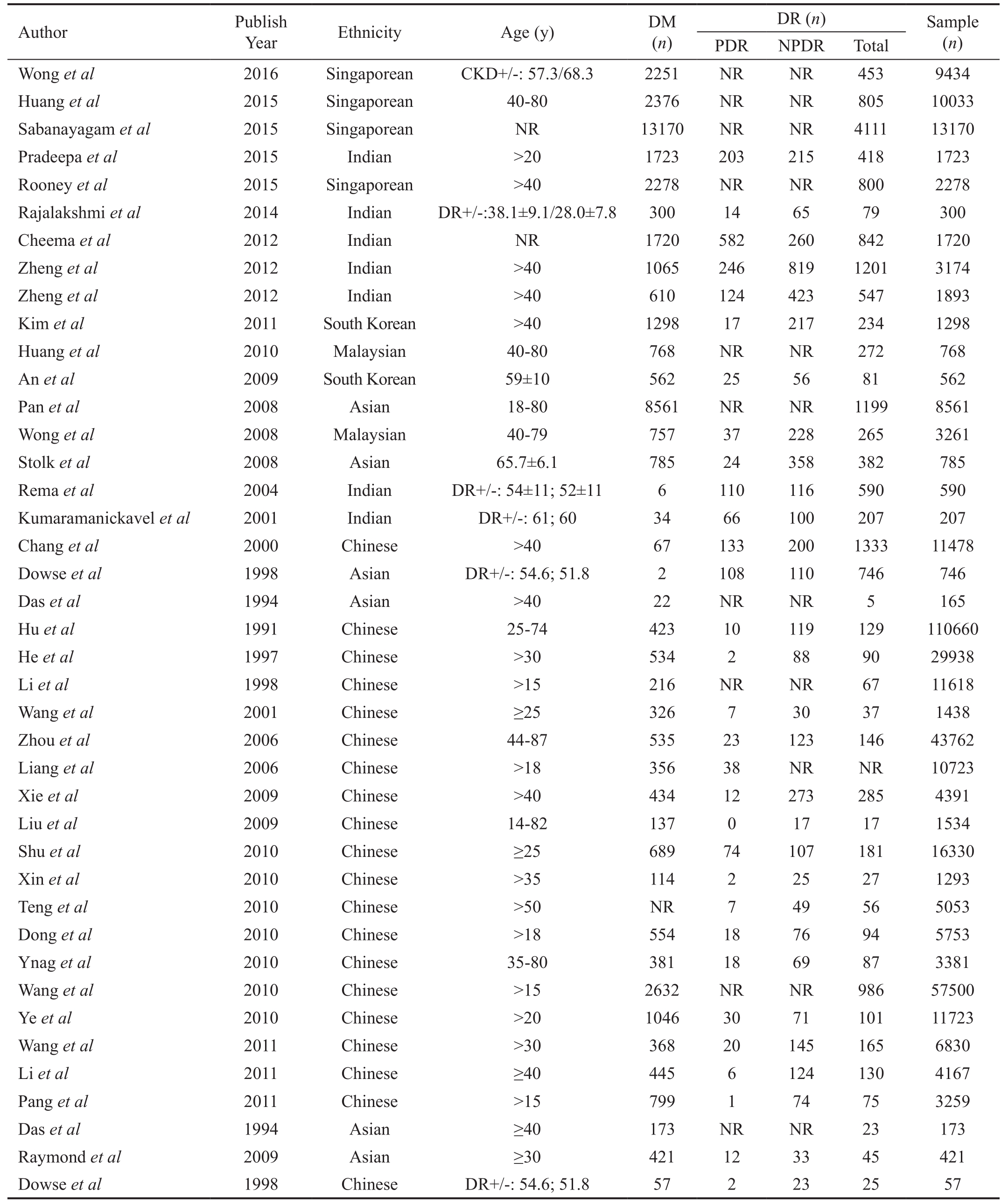
PDR: Proliferative diabetic retinopathy; NPDR: Nonproliferative diabetic retinopathy; DR: Diabetic retinopathy; DM: Diabetes mellitus;CKD+/-: Patients with/without CKD; DR+/-: Patients with/without DR.
Wong et al 2016 Singaporean CKD+/-: 57.3/68.3 2251 NR NR 453 9434 Huang et al 2015 Singaporean 40-80 2376 NR NR 805 10033 Sabanayagam et al 2015 Singaporean NR 13170 NR NR 4111 13170 Pradeepa et al 2015 Indian >20 1723 203 215 418 1723 Rooney et al 2015 Singaporean >40 2278 NR NR 800 2278 Rajalakshmi et al 2014 Indian DR+/-:38.1±9.1/28.0±7.8 300 14 65 79 300 Cheema et al 2012 Indian NR 1720 582 260 842 1720 Zheng et al 2012 Indian >40 1065 246 819 1201 3174 Zheng et al 2012 Indian >40 610 124 423 547 1893 Kim et al 2011 South Korean >40 1298 17 217 234 1298 Huang et al 2010 Malaysian 40-80 768 NR NR 272 768 An et al 2009 South Korean 59±10 562 25 56 81 562 Pan et al 2008 Asian 18-80 8561 NR NR 1199 8561 Wong et al 2008 Malaysian 40-79 757 37 228 265 3261 Stolk et al 2008 Asian 65.7±6.1 785 24 358 382 785 Rema et al 2004 Indian DR+/-: 54±11; 52±11 6 110 116 590 590 Kumaramanickavel et al 2001 Indian DR+/-: 61; 60 34 66 100 207 207 Chang et al 2000 Chinese >40 67 133 200 1333 11478 Dowse et al 1998 Asian DR+/-: 54.6; 51.8 2 108 110 746 746 Das et al 1994 Asian >40 22 NR NR 5 165 Hu et al 1991 Chinese 25-74 423 10 119 129 110660 He et al 1997 Chinese >30 534 2 88 90 29938 Li et al 1998 Chinese >15 216 NR NR 67 11618 Wang et al 2001 Chinese ≥25 326 7 30 37 1438 Zhou et al 2006 Chinese 44-87 535 23 123 146 43762 Liang et al 2006 Chinese >18 356 38 NR NR 10723 Xie et al 2009 Chinese >40 434 12 273 285 4391 Liu et al 2009 Chinese 14-82 137 0 17 17 1534 Shu et al 2010 Chinese ≥25 689 74 107 181 16330 Xin et al 2010 Chinese >35 114 2 25 27 1293 Teng et al 2010 Chinese >50 NR 7 49 56 5053 Dong et al 2010 Chinese >18 554 18 76 94 5753 Ynag et al 2010 Chinese 35-80 381 18 69 87 3381 Wang et al 2010 Chinese >15 2632 NR NR 986 57500 Ye et al 2010 Chinese >20 1046 30 71 101 11723 Wang et al 2011 Chinese >30 368 20 145 165 6830 Li et al 2011 Chinese ≥40 445 6 124 130 4167 Pang et al 2011 Chinese >15 799 1 74 75 3259 Das et al 1994 Asian ≥40 173 NR NR 23 173 Raymond et al 2009 Asian ≥30 421 12 33 45 421 Dowse et al 1998 Chinese DR+/-: 54.6; 51.8 57 2 23 25 57
The prevalence of NPDR in Asian T2DM patients was 27%(95%CI: 17%-38%). As to the prevalence of NPDR in various regions, our study showed that the prevalence of NPDR in Indian, South Korean, Malaysian, Asian and Chinese populations was 45% (95%CI: 13%-78%), 13% (95%CI: 7%-20%), 30% (95%CI: 27%-33%), 23% (95%CI: 2%-43%),22% (95%CI: 16%-27%), respectively, as shown in Table 3.
Table 2 The quality assessment according to the Newcastle Ottawa Quality Assessment Scale (NOQAS) of each study

 Wong et al 2016 4 2 3 9 Huang et al 2015 3 2 3 8 Sabanayagam et al 2015 3 2 3 8 Pradeepa et al 2015 4 2 3 9 Rooney et al 2015 3 2 3 8 Rajalakshmi et al 2014 3 2 3 8 Cheema et al 2012 3 2 3 8 Zheng et al 2012 3 2 3 8 Zheng et al 2012 3 2 2 7 Kim et al 2011 3 2 2 7 Huang et al 2010 3 2 3 8 An et al 2009 4 2 3 9 Pan et al 2008 3 2 2 7 Wong et al 2008 3 2 3 8 Stolk et al 2008 3 2 3 8 Rema et al 2004 3 2 2 7 Kumaramanickavel et al2001 3 2 3 8 Chang et al 2000 3 2 3 8 Dowse et al 1998 3 2 3 8 Das et al 1994 3 2 2 7 Hu et al 1991 3 2 3 8 He et al 1997 3 2 3 8 Li et al 1998 3 2 3 8 Wang et al 2001 3 2 2 7 Zhou et al 2006 3 2 3 8 Liang et al 2006 3 2 2 7 Xie et al 2009 3 2 2 7 Liu et al 2009 3 2 3 8 Shu et al 2010 3 2 3 8 Xin et al 2010 4 2 2 8 Teng et al 2010 4 2 3 9 Dong et al 2010 4 2 2 8 Ynag et al 2010 3 2 3 7 Wang et al 2010 3 2 3 8 Ye et al 2010 3 2 3 8 Wang et al 2011 4 2 2 8 Li et al 2011 3 2 3 8 Pang et al 2011 4 2 2 8 Das et al 1994 3 2 3 8 Raymond et al 2009 4 2 2 8 Dowse et al 1998 4 2 3 9
Wong et al 2016 4 2 3 9 Huang et al 2015 3 2 3 8 Sabanayagam et al 2015 3 2 3 8 Pradeepa et al 2015 4 2 3 9 Rooney et al 2015 3 2 3 8 Rajalakshmi et al 2014 3 2 3 8 Cheema et al 2012 3 2 3 8 Zheng et al 2012 3 2 3 8 Zheng et al 2012 3 2 2 7 Kim et al 2011 3 2 2 7 Huang et al 2010 3 2 3 8 An et al 2009 4 2 3 9 Pan et al 2008 3 2 2 7 Wong et al 2008 3 2 3 8 Stolk et al 2008 3 2 3 8 Rema et al 2004 3 2 2 7 Kumaramanickavel et al2001 3 2 3 8 Chang et al 2000 3 2 3 8 Dowse et al 1998 3 2 3 8 Das et al 1994 3 2 2 7 Hu et al 1991 3 2 3 8 He et al 1997 3 2 3 8 Li et al 1998 3 2 3 8 Wang et al 2001 3 2 2 7 Zhou et al 2006 3 2 3 8 Liang et al 2006 3 2 2 7 Xie et al 2009 3 2 2 7 Liu et al 2009 3 2 3 8 Shu et al 2010 3 2 3 8 Xin et al 2010 4 2 2 8 Teng et al 2010 4 2 3 9 Dong et al 2010 4 2 2 8 Ynag et al 2010 3 2 3 7 Wang et al 2010 3 2 3 8 Ye et al 2010 3 2 3 8 Wang et al 2011 4 2 2 8 Li et al 2011 3 2 3 8 Pang et al 2011 4 2 2 8 Das et al 1994 3 2 3 8 Raymond et al 2009 4 2 2 8 Dowse et al 1998 4 2 3 9
Regarding to the prevalence of PDR in DR patients, our study indicated that the prevalence of PDR overall Asian DR patients, Indian, South Korean, Malaysian, Asian and Chinese populations was 17% (95%CI: 13%-22%), 26% (95%CI: 17%-36%), 19% (95%CI: -5%-42%), 14% (95%CI: 10%-18%), 8%(95%CI: 1%-14%), and 15% (95%CI: 10%-20%), respectively(Table 3 and Figure 3).
Furthermore, NPDR was more common than PDR in either overall Asian DR patients, Indian, South Korean, Malaysian,Asian or Chinese populations as our pooled analysis and subgroup analysis showed that the prevalence of NPDR was 83% (95%CI: 78%-87%), 74% (95%CI: 64%-83%), 81%(95%CI: 58%-105%), 86% (95%CI: 82%-90%), 92% (95%CI:86%-99%), 85% (95%CI: 80%-90%), respectively.
Sensitivity Analysis and Publication Bias In addition, we performed the sensitivity analysis. The previous results were not affected by omission of any studies, suggesting that the results were relatively stable. Otherwise, we did not perform the publication bias due to the insufficient data.
DR is a leading complication of diabetes mellitus (DM),affecting over 130 million people worldwide[53]. Therefore,how to prevent the progression of DR and treat this devastating complication remains a challenge for ophthalmologists[54].DR is considered as an indicator of systemic diabetic microvascular complications, and also a crucial indicator of the impact of diabetes on patients[12]. It is well acknowledged that accurate prevalence of DR including PDR and NPDR in T2DM patients could be used for guiding public health education and managing the clinical aspects of this disease in a favorable way[55]. However, the prevalence of DR, PDR and NPDR in T2DM patients from various regions reported in several studies remains conflicting[16,21,26]. In addition, results from two previous Meta-analyses[11-12] were also controversial,suggesting that an updated Meta-analysis is necessary to provide ophthalmologists with more evidence to treat this disease. To the best of our knowledges, this systematic review and Meta-analysis was the fifirst study that investigated the prevalence of DR, PDR and NPDR in the Asian T2DM patients.
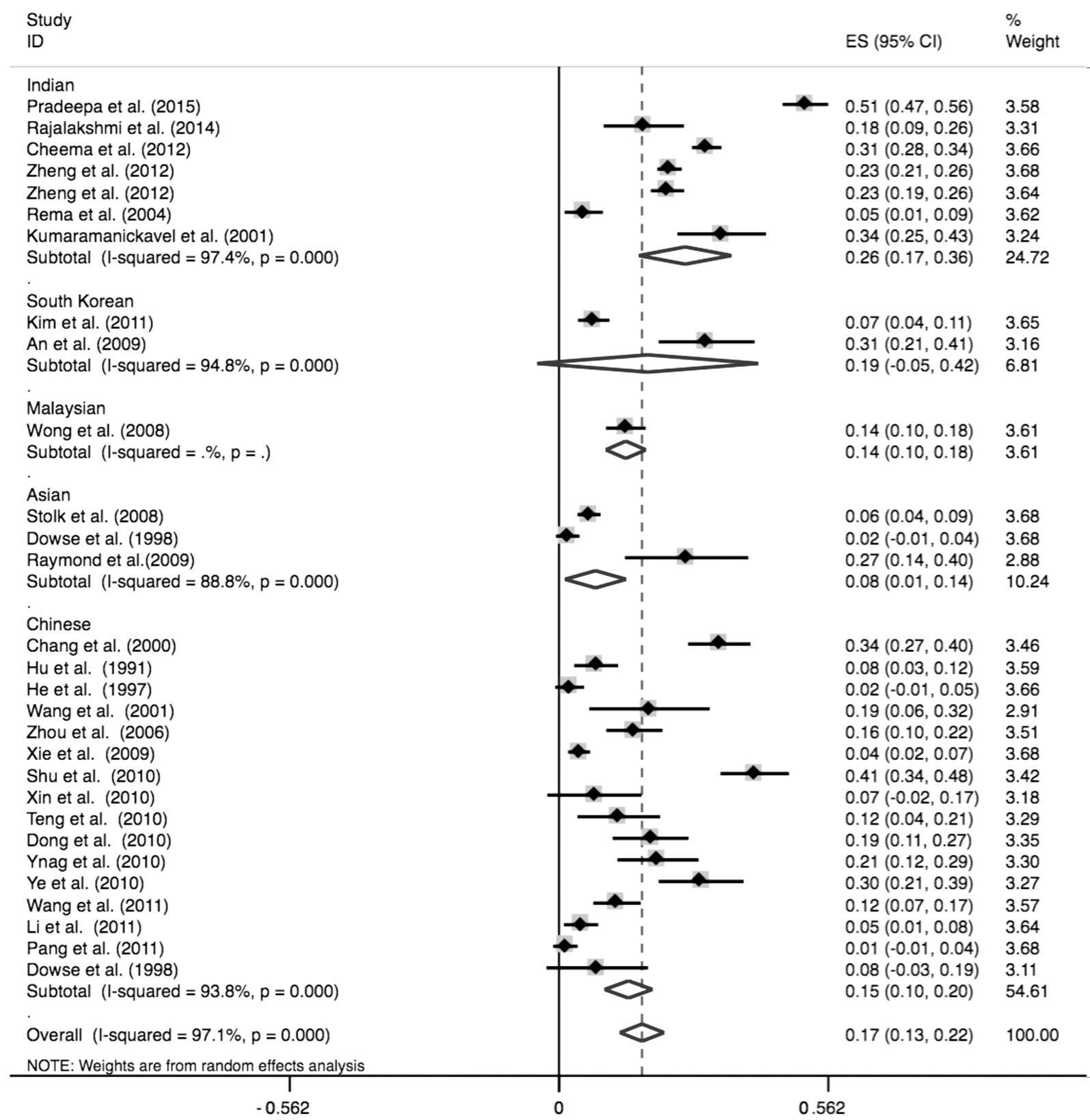
Figure 3 Forest plot of prevalence of PDR in Indian, South Korean, Malaysian, Asian and Chinese populations.
In our study, a total of 41 studies were finally included according to our inclusion and exclusion criteria. Our results showed that pooled prevalence of DR in Asian T2DM patients was 28%, which was consistent with several studies[22,24,56].In Tan et al's study[56], they recruited 2877 DM patients of Malay, Indian, and Chinese ethnicity aged 40 years older,living in Singapore. Their results indicated that the overall age-standardized prevalence (95%CI) was 28.2% (25.9%-30.6%) for any DR, which was consistent with our study,further suggesting that DR was a common complication among DM patients. Besides, according to our and Tan et al's study[56], more attention should be paid to DR prevention in the follow-up time if the patient was diagnosed as DM. However,controversial results were observed in other studies[15,26,30]. In An et al[30] and Pan et al[15]'s study, the prevalence of DR in T2DM was smaller than that in our study; while Cheema et al[26] reported that almost 49% of T2DM patients suffered from DR. In our opinion, several factors might be contributed to this difference. Fifirst, different sample size might be a primary contributor. Our study included 41 studies involving 17 336 DR and 48 995 DM individuals, which made our results more credible than these studies. Second, we conducted this pooled analysis, in which data in various studies were used, which might lead to the change of distribution of DR in T2DM patients. Besides, different follow-up time, various inclusion and exclusion criteria and measurement errors could also explain the difference between our results and An et al[30], Pan et al[15] and Cheema et al[26]'s study. Furthermore, our results were also different from Maroufizadeh et al[12] and Liu et al[11]'s Meta-analysis. In their study, the prevalence of DR in DM patients was 41.9% and 23%, respectively. In Maroufizadeh et al's study[12], thirty-one studies involving 23 729 patients with type 1 and 2 diabetes were included; and Liu et al[11] only recruited nineteen studies. Therefore, the numbers of included studies and the total sample size might be the most important factor for the difference between our results and theirs.Besides, Maroufizadeh et al[12] reported the prevalence of DR in both type 1 and 2 diabetes patients; therefore, it is easy for us to undefirstand this discrepancy. Therefore, our results were more credible than previous single-center studies and Meta-analysis, which could be used for guiding public health education and managing the clinical aspects of this disease in a favorable way.Regarding prevalence of PDR and NPDR, our Meta-analysis showed the prevalence of PDR and NPDR was 6% and 27% in Asian T2DM, and 17% and 83% in DR patients, respectively.Our results indicated that NPDR was more common than PDR in both T2DM and DR populations, suggesting that NPDR screening should be paid more attention compared with PDR screening. In addition, our results also verified that NPDR was the early stage in DR progression. NPDR screening and suitable intervention should be applied if possible in T2DM patients[57]. Furthermore, our results were also consistent with two previous studies with numerous sample size[31,56].
Tan et al[56] conducted a survey recruiting 2877 individuals,which showed prevalence of PDR and NPDR was 3.75%and 24.41%, respectively, further verifying the importance of NPDR screening in T2DM patients. Besides, different prevalence of PDR and NPDR in T2DM were reported in some other studies, though their study also indicated higher prevalence of NPDR in T2DM[24,26]. Dissimilarity of ophthalmologic definitions, examination methodologies and specific population might contribute to this difference. Our study was more credible than Cheema et al[26] and Pradeepaet al[24]'s study as they only performed the analysis in Indian populations; while our study was multi-ethnic. Furthermore,although two previous Meta-analyses[11-12] showed the same results as ours, their studies only focus on the prevalence PDR and NPDR in T2DM patients, while we performed analyses in both T2DM and DR patients. Therefore, based on our results and previous studies, we recommend that NPDR screening is essential in T2DM to prevent its progression into severe stage(PDR)[57].
Table 3 The pooled results of prevalence of DR, PDR and NPDR in patients with DM
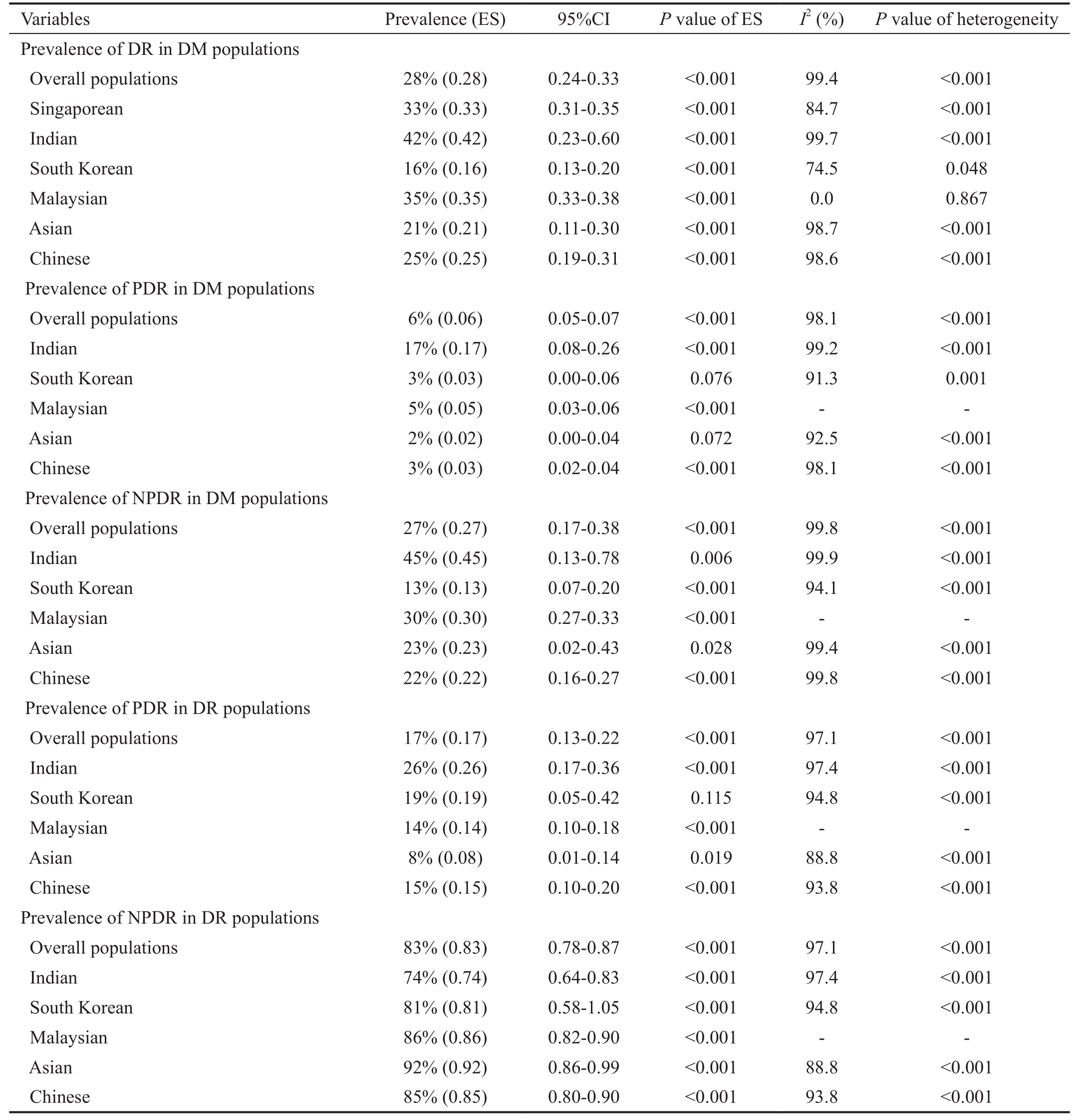
PDR: Proliferative diabetic retinopathy; NPDR: Nonproliferative diabetic retinopathy; DR: Diabetic retinopathy; DM: Diabetes mellitus; T2DM:Type 2 diabetes mellitus. Effect size with 95%CI was assessed to analyze the pooled prevalence of DR, PDR and NPDR in T2DM populations.P<0.05 was considered as statistically significant.
Prevalence of DR in DM populations Overall populations 28% (0.28) 0.24-0.33 <0.001 99.4 <0.001 Singaporean 33% (0.33) 0.31-0.35 <0.001 84.7 <0.001 Indian 42% (0.42) 0.23-0.60 <0.001 99.7 <0.001 South Korean 16% (0.16) 0.13-0.20 <0.001 74.5 0.048 Malaysian 35% (0.35) 0.33-0.38 <0.001 0.0 0.867 Asian 21% (0.21) 0.11-0.30 <0.001 98.7 <0.001 Chinese 25% (0.25) 0.19-0.31 <0.001 98.6 <0.001 Prevalence of PDR in DM populations Overall populations 6% (0.06) 0.05-0.07 <0.001 98.1 <0.001 Indian 17% (0.17) 0.08-0.26 <0.001 99.2 <0.001 South Korean 3% (0.03) 0.00-0.06 0.076 91.3 0.001 Malaysian 5% (0.05) 0.03-0.06 <0.001 - -Asian 2% (0.02) 0.00-0.04 0.072 92.5 <0.001 Chinese 3% (0.03) 0.02-0.04 <0.001 98.1 <0.001 Prevalence of NPDR in DM populations Overall populations 27% (0.27) 0.17-0.38 <0.001 99.8 <0.001 Indian 45% (0.45) 0.13-0.78 0.006 99.9 <0.001 South Korean 13% (0.13) 0.07-0.20 <0.001 94.1 <0.001 Malaysian 30% (0.30) 0.27-0.33 <0.001 - -Asian 23% (0.23) 0.02-0.43 0.028 99.4 <0.001 Chinese 22% (0.22) 0.16-0.27 <0.001 99.8 <0.001 Prevalence of PDR in DR populations Overall populations 17% (0.17) 0.13-0.22 <0.001 97.1 <0.001 Indian 26% (0.26) 0.17-0.36 <0.001 97.4 <0.001 South Korean 19% (0.19) 0.05-0.42 0.115 94.8 <0.001 Malaysian 14% (0.14) 0.10-0.18 <0.001 - -Asian 8% (0.08) 0.01-0.14 0.019 88.8 <0.001 Chinese 15% (0.15) 0.10-0.20 <0.001 93.8 <0.001 Prevalence of NPDR in DR populations Overall populations 83% (0.83) 0.78-0.87 <0.001 97.1 <0.001 Indian 74% (0.74) 0.64-0.83 <0.001 97.4 <0.001 South Korean 81% (0.81) 0.58-1.05 <0.001 94.8 <0.001 Malaysian 86% (0.86) 0.82-0.90 <0.001 - -Asian 92% (0.92) 0.86-0.99 <0.001 88.8 <0.001 Chinese 85% (0.85) 0.80-0.90 <0.001 93.8 <0.001
We also performed a subgroup analysis to explore whether the prevalence of DR, PDR and NPDR in T2DM is different among various origins. Our subgroup analysis showed that the prevalence of PDR in Indian patients with T2DM and DR was the highest compared with that in Southern Korean, Malaysian,Asian and Chinese populations. Meanwhile, some researchers held the views that Indian ethnicity was an independent risk factor for DR[56], further verifying our results. Therefore, as to Indian ophthalmologists, more focus should be paid on Indian T2DM patients than ophthalmologists from other origins. In our views, the different prevalence in various origins might be resulted from obesity, urbanization, changes in diet, education level of the involved region, increasingly sedentary lifestyles and so on[58]. In addition, the characteristics of studies, such as different inclusion and exclusion criteria, measurement errors and sample size might also contribute to the discrepancy of prevalence between different origins. Therefore, improvement of education, diet and other factors should also gain enough attentions other than regular examinations in T2DM to prevent the occurrence of this complication.
Our study is the fifirst systematic review and Meta-analysis that investigated the prevalence of DR, PDR and NPDR in T2DM patients in various Asian countries. Although our study provided basic evidence for ophthalmologists in DR screening, some limitations should be addressed. Fifirst, our study only focused on the prevalence in Asian DM patients due to the insufficient data in other ethnicities. Therefore,whether the prevalence of DR, PDR and NPDR in Caucasian populations was as high as that in Asian populations remains further investigated. Second, the prevalence might be affected by other risk factors, such as diet and environment. Due to the insufficient data, we could not perform adjusted analysis in our study, which is also a limitation. Third, sample size in some studies was relatively small, which might also have impacts on our pooled results. Therefore, studies with large sample size in different ethnicities should be performed to determinate the accurate prevalence of DR, PDR and NPDR to provide more knowledges to ophthalmologists when they treat T2DM patients diagnosed as DR.
In either T2DM Asian patients or DR patients, NPDR was more common than PDR. Based on our results, we should pay more attention to NPDR screening and management in T2DM patients, and we also recommend suitable interventions to prevent its progression. In addition, other factors, such as diet and environment should also not be ignored.
Conflicts of Interest:Yang QH, None; Zhang Y, None;Zhang XM, None; Li XR, None.
1 NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016;387(10027):1513-1530.
2 Hod M, Kapur A, Sacks DA, Hadar E, Agarwal M, di Renzo GC, Roura LC, McIntyre HD, Morris JL, Divakar H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: a pragmatic guide for diagnosis, management, and care. Int J Gynaecol Obstet 2015;131:S173-S211.
3 Vinik AI, Nevoret ML, Casellini C, Parson H. Diabetic neuropathy.Endocrinol Metab Clin North Am 2013;42(4):747-787.
4 Kayama Y, Raaz U, Jagger A, Adam M, Schellinger IN, Sakamoto M,Suzuki H, Toyama K, Spin JM, Tsao PS. Diabetic cardiovascular disease induced by oxidative stress. Int J Mol Sci 2015;16(10):25234-25263.
5 Yamagishi S, Imaizumi T. Diabetic vascular complications: pathophysiology,biochemical basis and potential therapeutic strategy. Curr Pharm Des 2005;11(18):2279-2299.
6 Hammes HP. Diabetic retinopathy: hyperglycaemia, oxidative stress and beyond. Diabetologia 2018;61(1):29-38.
7 Wang LZ, Cheung CY, Tapp RJ, Hamzah H, Tan G, Ting D, Lamoureux E, Wong TY. Availability and variability in guidelines on diabetic retinopathy screening in Asian countries. Br J Ophthalmol 2017;101(10):1352-1360.
8 Huang OS, Tay WT, Ong PG, Sabanayagam C, Cheng CY, Tan GS,Cheung GC, Lamoureux EL, Wong TY. Prevalence and determinants of undiagnosed diabetic retinopathy and vision-threatening retinopathy in a multiethnic Asian cohort: the Singapore Epidemiology of Eye Diseases(SEED) study. Br J Ophthalmol 2015;99(12):1614-1621.
9 Thomas RL, Distiller L, Luzio SD, Chowdhury SR, Melville VJ,Kramer B, Owens DR. Ethnic differences in the prevalence of diabetic retinopathy in persons with diabetes when first presenting at a diabetes clinic in South Africa. Diabetes Care 2013;36(2):336-341.
10 Stolk RP, van Schooneveld MJ, Cruickshank JK, Hughes AD, Stanton A, Lu JM, Patel A, Thom SA, Grobbee DE, Vingerling JR, AdRem Project Team and ADVANCE Management Committee. Retinal vascular lesions in patients of Caucasian and Asian origin with type 2 diabetes:baseline results from the ADVANCE Retinal Measurements (AdRem)study. Diabetes Care 2008;31(4):708-713.
11 Liu L, Wu XM, Liu LM, Geng J, Yuan Z, Shan ZY, Chen L. Prevalence of diabetic retinopathy in mainland China: a meta-analysis. PLoS One 2012;7(9):e45264.
12 Maroufizadeh S, Almasi-Hashiani A, Hosseini M, Sepidarkish M,Omani Samani R. Prevalence of diabetic retinopathy in Iran: a systematic review and Meta-analysis. Int J Ophthalmol 2017;10(5):782-789.
13 Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010;25(9):603-605.
14 Huang OS, Lamoureux EL, Tay WT, Tai ES, Wang JJ, Wong TY.Glycemic and blood pressure control in an Asian malay population with diabetes and diabetic retinopathy. Arch Ophthalmol 2010;128(9):1185-1190.
15 Pan CY, Ho LT, Soegondo S, Prodjosudjadi W, Suwanwalaikorn S,Lim SC, Chan TM, Chow KW, Thoenes M, Choi DS, DEMAND Study Investigators. Prevalence of albuminuria and cardiovascular risk profile in a referred cohort of patients with type 2 diabetes: an Asian perspective.Diabetes Technol Ther 2008;10(5):397-403.
16 Kumaramanickavel G, Sripriya S, Vellanki RN, Upadyay NK,Badrinath SS, Arokiasamy T, Sukumar B, Vidhya A, Joseph B,Sharma T, Gopal L. Tumor necrosis factor allelic polymorphism with diabetic retinopathy in India. Diabetes Res Clin Pract 2001;54(2):89-94.
17 Das BN, Thompson JR, Patel R, Rosenthal AR. The prevalence of eye disease in Leicester: a comparison of adults of Asian and European descent. J R Soc Med 1994;87(4):219-222.
18 Raymond NT, Varadhan L, Reynold DR, Bush K, Sankaranarayanan S, Bellary S, Barnett AH, Kumar S, O'Hare JP, UK Asian Diabetes Study Retinopathy Study Group. Higher prevalence of retinopathy in diabetic patients of South Asian ethnicity compared with white Europeans in the community: a cross-sectional study. Diabetes Care 2009;32(3):410-415.
19 Dowse GK, Humphrey AR, Collins VR, Plehwe W, Gareeboo H,Fareed D, Hemraj F, Taylor HR, Tuomilehto J, Alberti KG, Zimmet PZ.Prevalence and risk factors for diabetic retinopathy in the multiethnic population of Mauritius. Am J Epidemiol 1998;147(5):448-457.
20 Cheung CY, Sabanayagam C, Law AK, Kumari N, Ting DS, Tan G, Mitchell P, Cheng CY, Wong TY. Retinal vascular geometry and 6 year incidence and progression of diabetic retinopathy. Diabetologia 2017;60(9):1770-1781.
21 Wong CW, Lamoureux EL, Cheng CY, Cheung GC, Tai ES, Wong TY,Sabanayagam C. Increased burden of vision impairment and eye diseases in persons with chronic kidney disease - a population-based study.EBioMedicine 2016;5:193-197.
22 Sabanayagam C, Khoo EY, Lye WK, Ikram MK, Lamoureux EL,Cheng CY, Tan ML, Salim A, Lee J, Lim SC, Tavintharan S, Thai AC,Heng D, Ma S, Tai ES, Wong TY. Diagnosis of diabetes mellitus using HbA1c in Asians: relationship between HbA1c and retinopathy in a multiethnic Asian population. J Clin Endocrinol Metab 2015;100(2):689-696.
23 Rooney D, Lye WK, Tan G, Lamoureux EL, Ikram MK, Cheng CY,Kumari N, Zheng YF, Mitchell P, Wang JJ, Wong TY, Sabanayagam C.Body mass index and retinopathy in Asian populations with diabetes mellitus. Acta Diabetol 2015;52(1):73-80.
24 Pradeepa R, Surendar J, Indulekha K, Chella S, Anjana RM, Mohan V.Relationship of diabetic retinopathy with coronary artery disease in Asian Indians with type 2 diabetes: the Chennai Urban Rural Epidemiology Study (CURES) Eye Study: 3. Diabetes Technol Ther 2015;17(2):112-118.
25 Rajalakshmi R, Amutha A, Ranjani H, Ali MK, Unnikrishnan R,Anjana RM, Narayan KM, Mohan V. Prevalence and risk factors for diabetic retinopathy in Asian Indians with young onset type 1 and type 2 diabetes. J Diabetes Complicat 2014;28(3):291-297.
26 Cheema BS, kohli HS, Sharma R, Bhansali A, Khullar M. Endothelial nitric oxide synthase gene polymorphism and type 2 diabetic retinopathy among Asian Indians. Acta Diabetol 2012;49(6):481-488.
27 Zheng YF, Lamoureux EL, Ikram MK, Mitchell P, Wang JJ, Younan C, Anuar AR, Tai ES, Wong TY. Impact of migration and acculturation on prevalence of type 2 diabetes and related eye complications in Indians living in a newly urbanised society. PLoS One 2012;7(4):e34829.
28 Zheng YF, Lamoureux EL, Chiang PC, Anuar AR, Ding J, Wang JJ,Mitchell P, Tai ES, Wong TY. Language barrier and its relationship to diabetes and diabetic retinopathy. BMC Public Health 2012;12:781.
29 Kim JH, Kwon HS, Park YM, Lee JH, Kim MS, Yoon KH, Lee WC, Cha BY, Son HY. Prevalence and associated factors of diabetic retinopathy in rural Korea: the Chungju metabolic disease cohort study. J Korean Med Sci 2011;26(8):1068-1073.
30 An JH, Cho YM, Yu HG, Jang HC, Park KS, Kim SY, Lee HK. The clinical characteristics of normoalbuminuric renal insufficiency in Korean type 2 diabetic patients: a possible early stage renal complication. J Korean Med Sci 2009;24(Suppl):S75-S81.
31 Wong TY, Cheung N, Tay WT, Wang JJ, Aung T, Saw SM, Lim SC,Tai ES, Mitchell P. Prevalence and risk factors for diabetic retinopathy:the Singapore Malay Eye Study. Ophthalmology 2008;115(11):1869-1875.
32 Chang C, Lu F, Yang YC, Wu JS, Wu TJ, Chen MS, Chuang LM, Tai TY. Epidemiologic study of type 2 diabetes in Taiwan. Diabetes Res Clin Pract 2000;50(Suppl 2):S49-S59.
33 Hu YH, Pan XR, Liu PA, Li GW, Howard BV, Bennett PH. Coronary heart disease and diabetic retinopathy in newly diagnosed diabetes in Da Qing, China: the Da Qing IGT and Diabetes Study. Acta Diabetol 1991;28(2):169-173.
34 He S, Guo Y, Li Z. Epidemiologic study of diabetic retinopathy in Capital Steel Company. Zhonghua Yan Ke Za Zhi 1997;33(5):381-383.
35 Li SL, Zhou YF, Chen D, Yang MG, Zhu ML. Epidemiological investigation of diabetic retinopathy risk factors. Chin J Ocul Fundus Dis 1998;14:119-121.
36 Wang GL, Zhang F, Yuan SY, et al. A screening survey of diabetic retinopathy and other chronic complications in beijing district.Ophthalmology In China 2001;10:180-182.
37 Zou HD, Zhang X, Zhu JF, et al. Epidemiological investigation of diabetic retinopathy in Beixinjing blocks, Shanghai. Chin J Ocul Fundus Dis 2006;22:31-34.
38 Liang XJ, Lin JJ, Huang Z, Li GP, Wu XY. Prevalence and risk factors of diabetic retinopathy in foshan city. Guangdong Medical Journal 2006;27:1552-1553.
39 Xie XW, Xu L, Yang H, Wang S, Jonas JB. Frequency of diabetic retinopathy in the adult population in China: the Beijing Eye Study 2001.Int Ophthalmol 2009;29(6):485-493.
40 Liu L, Chen L, Hu YD, Liu LM. Analysis risk factors for diabetic retinopathy. Shandong Medical Journal 2009;49:52-53.
41 Shu XW, Wang Y, Fan CF, Sheng YJ, Zhang H, Wu CL. Epidemiology study on the prevalence rate and risk factors of diabetic retinopathy in rural residents in shandong. Chin J Ocul Fundus Dis 2010;26:113-115.
42 Ye XQ. The analysis about epidemiological survey of diabetic retinopathy in huizhou city. Guide of China Medicine 2010;8:27-28.
43 Teng Y, Cui H, Zhang QS, Teng YF, Su Y, Yang MM, Yu XH.Prevalence of diabetic retinopathy among the elderly in rural southern Shuangcheng City, Heilongjiang Province. Zhonghua Liu Xing Bing Xue Za Zhi 2010;31(8):856-859.
44 Dong HL. Screening procession for diabetic retinopathy for Shunyi district Houshayu valley residents. . Medical Information 2010;10:2701-2702.
45 Yang MZ, Wei SQ. Early detection for diabetic retinopathy in grassroots community and results analysis. Hebei Medical Journal 2010;32:844-845.
46 Wang HB, Sun FX, Zhang Q, Zhai M, Wang SF, Lu H. Epidemiologic study on the prevalence rate and risk factors of diabetic retinopathy in eastern countryside of Changzhi. . Chin J Ocul Fundus Dis 2010;26:109-112.
47 Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, Chen SJ, Dekker JM, Fletcher A, Grauslund J, Haffner S, Hamman RF,Ikram MK, Kayama T, Klein BE, Klein R, Krishnaiah S, Mayurasakorn K, O'Hare JP, Orchard TJ, Porta M, Rema MH, Roy MS, Sharma T,Shaw J, Taylor H, Tielsch JM, Varma R, Wang JJ, Wang NL, West S, Xu L, Yasuda M, Zhang XZ, Mitchell P, Wong TY, Meta-Analysis for Eye Disease (META-EYE) Study Group. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012;35(3):556-564.
48 Wang FH, Liang YB, Peng XY, Wang JJ, Zhang F, Wei WB, Sun LP,Friedman DS, Wang NL, Wong TY, Handan Eye Study Group. Risk factors for diabetic retinopathy in a rural Chinese population with type 2 diabetes: the Handan Eye Study. Acta Ophthalmol 2011;89(4):e336-e343.
49 Li BZ, Liu YL, Han L, et al. Epidemiological survey of diabetic retinopathy in shunyi district of beijing. Chin J Exp Ophthalmol 2011;29:747-752.
50 Pang C, Jia LL, Jiang SF, Liu W, Hou XH, Zuo YH, Gu HL, Bao YQ,Wu Q, Xiang KS, Gao X, Jia WP. Determination of diabetic retinopathy prevalence and associated risk factors in Chinese diabetic and pre-diabetic subjects: Shanghai diabetic complications study. Diabetes Metab Res Rev 2012;28(3):276-283.
51 Rema MH, Mohan V, Deepa R, Ravikumar R, Chennai Urban Rural Epidemiology Study-2. Association of carotid intima-media thickness and arterial stiffness with diabetic retinopathy: the Chennai Urban Rural Epidemiology Study (CURES-2). Diabetes Care 2004;27(8):1962-1967.
52 Pang C, Jia LL, Jiang SF, Liu W, Hou XH, Zuo YH, Gu HL, Bao YQ,Wu Q, Xiang KS, Gao X, Jia WP. Determination of diabetic retinopathy prevalence and associated risk factors in Chinese diabetic and pre-diabetic subjects: Shanghai diabetic complications study. Diabetes Metab Res Rev 2012;28(3):276-283.
53 Zaghloul H, Pallayova M, Al-Nuaimi O, Hovis KR, Taheri S.Association between diabetes mellitus and olfactory dysfunction: current perspectives and future directions. Diabet Med 2018;35(1):41-52.
54 Jin PY, Peng JJ, Zou HD, Wang WW, Fu J, Shen BJ, Bai XL, Xu X,Zhang X. A five-year prospective study of diabetic retinopathy progression in Chinese type 2 diabetes patients with “well-controlled” blood glucose.PLoS One 2015;10(4):e0123449.
55 Askew DA, Crossland L, Ware RS, Begg S, Cranstoun P, Mitchell P,Jackson CL. Diabetic retinopathy screening and monitoring of early stage disease in general practice: design and methods. Contemp Clin Trials 2012;33(5):969-975.
56 Tan GS, Gan A, Sabanayagam C, Tham YC, Neelam K, Mitchell P,Wang JJ, Lamoureux EL, Cheng CY, Wong TY. Ethnic differences in the prevalence and risk factors of diabetic retinopathy: the singapore epidemiology of eye diseases study. Ophthalmology 2018;125(4):529-536.
57 Panagiotoglou T, Tsilimbaris M, Ginis H, Karyotakis N, Georgiou V, Koutentakis P, Pallikaris I. Ocular rigidity and outflow facility in nonproliferative diabetic retinopathy. J Diabetes Res 2015;2015:141598.
58 Sivaprasad S, Gupta B, Crosby-Nwaobi R, Evans J. Prevalence of diabetic retinopathy in various ethnic groups: a worldwide perspective.Surv Ophthalmol 2012;57(4):347-370.