
Citation: Zhao KK, Yang Y, Wang H, Li L, Wang ZY, Jiang
F, Qu JF. Axial length/corneal radius of curvature ratio and refractive
development evaluation in 3- to 4-year-old children: the Shanghai Pudong Eye
Study. Int J Ophthalmol
2019;12(6):1021-1026
DOI:10.18240/ijo.2019.06.23
・Investigation・
Axial length/corneal radius of curvature
ratio and refractive development evaluation in 3- to 4-year-old children: the
Shanghai Pudong Eye Study
Ke-Ke Zhao1,
Yuan Yang2,3, Hong Wang1, Lu Li1, Zhao-Yang
Wang2,3, Fan Jiang1, Ji-Fang Qu1
1Shanghai Children’s Medical Center, Shanghai Jiao
Tong University School of Medicine, Shanghai 200127, China
2Shanghai Ninth People’s Hospital, Shanghai Jiao Tong
University School of Medicine, Shanghai 200011, China
3Shanghai Key Laboratory of Orbital Diseases and
Ocular Oncology, Shanghai 200011, China
Co-first authors: Ke-Ke Zhao and Yuan Yang
Correspondence to: Fan Jiang and Ji-Fang
Qu. Shanghai Children’s Medical Center, Shanghai Jiao Tong University School of
Medicine, Shanghai 200127, China. fanjiang@shsmu.edu.cn; rachelqu@163.com
Received:
Abstract
AIM: To measure and
analysis axial length (AL)/corneal radius of curvature (CRC) ratio and other
refractive parameters, provide a medical reference range for refractive
development evaluation and earlier visual impairment screening of 3 to 4y
kindergarten students.
METHODS: Between April and
June 2017, a total of 4350 participants aged 3- to 4-year-old (8700 eyes) from
10 cluster random sampling kindergartens in Shanghai, Pudong District were
involved. According to the measurement and analysis of the unaided visual
acuity (VA), AL, CRC, AL/CRC ratio, astigmatism and other refractive
parameters, the data distribution and reference range were obtained.
RESULTS: Uncorrected VA of
examined children was 0.23±0.08 (logMAR, mean±SD) [95% confidence interval (CI)
range ≤0.36]; AL was 22.10±
CONCLUSION:
VA and AL/CRC ratio reference could be used to assess refractive
development in children and screening uncorrected refractive errors or
amblyopia. Astigmatism needs to be considered in the diagnosis.
KEYWORDS: children; axial length/corneal radius of curvature ratio; refractive
development; visual impairment; reference
DOI:10.18240/ijo.2019.06.23
Citation: Zhao KK, Yang Y, Wang H, Li L, Wang ZY, Jiang
F, Qu JF. Axial length/corneal radius of curvature ratio and refractive
development evaluation in 3- to 4-year-old children: the Shanghai Pudong Eye
Study. Int J Ophthalmol
2019;12(6):1021-1026
INTRODUCTION
Recent population-based studies have revealed that
the most frequent cause of irreversible visual impairment and blindness in
China was degenerative myopia[1-6].
Because of the detection failure, children with refractive errors are easily to
be ignored and stayed unnoticed for years, which will lead to severe decrease
in visual acuity (VA). Since 3 years of age is a sensitive period for visual
development, any alternation in the developing brain can leads to permanent
visual loss in the affected eye[7]. The United
States Preventive Services Task Force (USPSTF) recommends vision screening for
all children at least once between the ages of 3 and 5 years[7].
Identification, diagnosis and treatment of visual impairment before
school entry could help improve VA outcomes for children with vision disorders,
and reduce the prevalence of refractive errors in the population[8-10].
Cycloplegic refraction is considered to be the golden
standard for pediatric refractive errors diagnosis[11].
However, accurate technical requirement for environment and examiners, lack of
cooperation with children and long inspection time limiting its application in
vision impairment screening[12]. Effective
strategies are needed to assess refractive development in children and
diagnosis uncorrected refractive errors. Axial length (AL) grows while corneal
radius of curvature (CRC) flattens in the process of emmetropization. A
previous study revealed that the correlation between spherical equivalent (SE)
and AL/CRC is stronger than that between AL or CRC alone, which suggests that
AL/CRC may be a potential reference for refractive error, especially when
cycloplegic refraction is unavailable in children[13].
This Pudong school-based, cross-sectional study
involved 4350 kindergarten students aged 3 to 4y. All the participants were
examined by ophthalmologists with comprehensive ocular examinations, including
distance VA (without spectacles, if worn), noncycloplegic autorefraction,
ocular biometric measurement and ocular movement examination. According to the
measurement and analysis of the unaided VA, AL, CRC, AL/CRC ratio and other
refractive parameters, obtained the mean value and 95% confidence interval
(CI), which will provide a medical reference range of 3 to 4y kindergarten
students and make visual impairments screening more effective and practical.
SUBJECTS AND METHODS
Ethical Approval
The study adhered to the tenets of the Declaration of Helsinki. Ethics
Committee approval was obtained from the Shanghai Children’s Medical Center
review board, and written informed consent was obtained from all subjects’
parents.
Populations
Shanghai, one of four municipalities under the direct jurisdiction of
China’s central government, is the financial capital of China, with a
population of 24.15 million[14]. The Pudong new
district, one of 17 administrative districts in Shanghai with both the maximum
land area (
Sample Selection
Cluster random sampling was used to select the study sample. According to
the geographical position, the education bureau has set up four education
departments in charge of all schools in Pudong new district. All 188
kindergartens were fairly subdivided and managed by four government education
departments[16]. Ten kindergartens of each
education department were selected for the study, a total of 40, by random
sampling of statistical software (SPSS for Windows, version 22.0; IBM-SPSS,
Chicago, IL, USA). The eligible students were 3 to 4 years of age, which have
been living in Pudong district for at least half a year and will continue to
live there for at least 5y. Children with ocular position abnormality,
nystagmus and other diseases of the anterior and posterior segment were
excluded.
Quality Control Procedures With the support of the
local government, principals and teachers of each kindergarten, quality control
procedures were implemented throughout the entire study. All examinations were
performed based on the standard operating procedure by one clinical team
between April and June, 2017. Five well-trained optometrists and
ophthalmologists were in charge of ocular examinations respectively during the
whole screening. Examinations were implemented in kindergartens, during the
week while classes were in session. All data was verified after double data
entry and analyzed by blinded statistician.
Ocular Examinations
Distance visual acuity VA was measured both
with and without spectacles, using a retroilluminated logarithm of the minimum
angle of resolution (logMAR) chart with tumbling-E optotypes (Precision Vision,
La Salle, IL, USA) at a distance of
Noncycloplegic autorefraction An autorefractor (KR
8800, Topcon Corp, Tokyo, Japan) was used to measure for their refractive
status and CRC without cycloplegic. After alignment, three repeated
measurements for each children and machine-calculated an average value.
Ocular biometric measurement AL was measured by IOL
Master (Carl Zeiss Meditec AG, Jena, Germany). Three repeated measurements were
taken and averaged. AL/CRC was calculated by statistical software.
Ocular movements
Students were asked to follow a moving penlight without moving their heads.
Nine directions of gaze were examined and recorded, including primary (straight
ahead), secondary (right, up, left, and down), and tertiary (upper right, lower
right, upper left and lower left).
Statistical Analysis All data were
independently entered into the database with Epidata software (version 3.1, The
Epidata Association, Odense, Denmark) by two individuals. Statistical analysis
was performed by SPSS software (SPSS for Windows, version 22.0; IBM-SPSS,
Chicago, IL, USA)[17]. Qualitative data were
expressed by frequency (percentage). Quantitative data were validated by
normality. For continuous traits, t-tests model will be used, both
person-specific and eye-specific analyses will be conducted. 95%CIs were
calculated[2]. The P value <0.05 was
statistically significant.
RESULTS
During the period from April to June 2017, 4350
participants (8700 eyes) were examined and completed at least one test at
ocular examination station. Distance VA was measured in 4313 (99.15%) students.
Noncycloplegic autorefraction examinations were available in 4342 (99.82%)
students. Ocular biometric measurement was completed in 4340 (99.77%) students.
All participants did ocular movements test. The age range of students was 3-4y.
The 47.69% of the students were female and 52.31% were male.
VA, AL, CRC and AL/CRC were obeyed normal
distribution, paired sample t-test
was used to compare refractive parameters between two eyes. In this sample,
statistical difference of VA was in right and left eyes (Table 1). Therefore
only data for right eyes were used for analysis of VA. There were no
significant differences between two eyes of AL, CRC, AL/CRC.
Table 1 Refractive parameters comparison of two eyes
by paired sample t-test in the Shanghai Pudong Eye Study
|
Factors |
Right eye |
Left eye |
P |
||
|
n |
Mean±SD |
n |
Mean±SD |
||
|
VA, logMAR |
4278 |
0.225±0.081 |
4276 |
0.228±0.086 |
|
|
AL, mm |
4339 |
22.102±0.662 |
4338 |
22.099±0.900 |
0.760 |
|
CRC, mm |
4341 |
7.859±0.260 |
4339 |
7.862±0.262 |
0.076 |
|
AL/CRC |
4337 |
2.812±0.102 |
4340 |
2.810±0.128 |
0.268 |
VA: Visual acuity; AL: Axial length; CRC: Corneal
radius of curvature. aP<0.05.
VA findings are presented in Figure
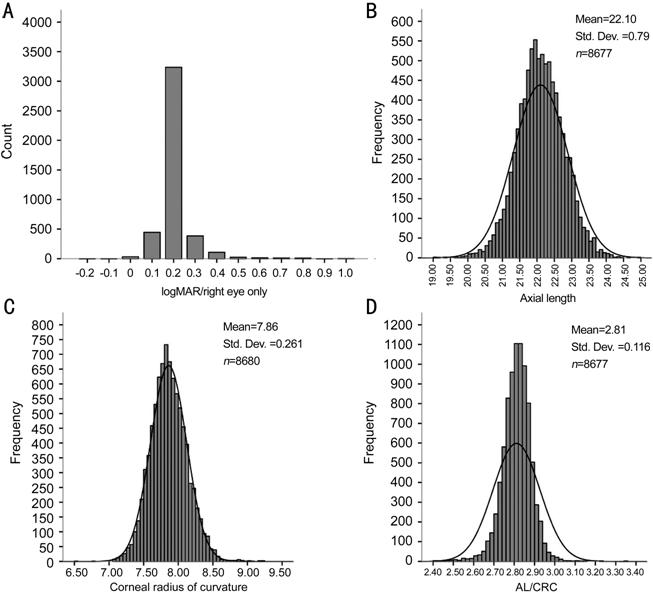
Figure 1 Refractive parameters distribution of the
participants in the Shanghai Pudong Eye Study A: Distribution of uncorrected VA
(logMAR) in 4278 measured right eyes. Statistical difference of VA was in right
and left eyes. Therefore, only data for right eyes were used for analysis of
VA. B: Distribution of AL in 8677 measured eyes; C: Distribution of CRC in 8680
measured eyes; D: Distribution of AL/CRC in 8677 measured eyes. VA, AL, CRC and
AL/CRC were obeyed normal distribution.
Table 2 Refractive parameters distribution of 3 to 4y
students in the Shanghai Pudong Eye Study
|
Factors |
Measured eyes (n) |
Range |
Median |
Mean±SD |
95%CI |
|
|
Lower bound |
Upper bound |
|||||
|
VA (R) |
|
-0.2-1.0 |
0.22 |
0.23±0.08 |
- |
0.36 |
|
VA (L) |
|
-0.1-1.0 |
0.22 |
0.23±0.09 |
- |
0.38 |
|
AL |
8677 |
18.83-24.90 |
22.09 |
22.10±0.79 |
20.55 |
23.65 |
|
CRC |
8680 |
6.55-9.24 |
7.85 |
7.86±0.26 |
7.35 |
8.37 |
|
AL/CRC |
8677 |
2.27-3.35 |
2.82 |
2.81±0.12 |
2.57 |
3.05 |
VA: Visual acuity; AL: Axial length; CRC: Corneal
radius of curvature; CI: Confidence interval. aStatistical
difference of VA was in right and left eyes.
According to autorefraction results, astigmatism was
characterized by skewed distribution, ranged -8.00 D to 0 D with median -0.50
D. As illustrated in Figure
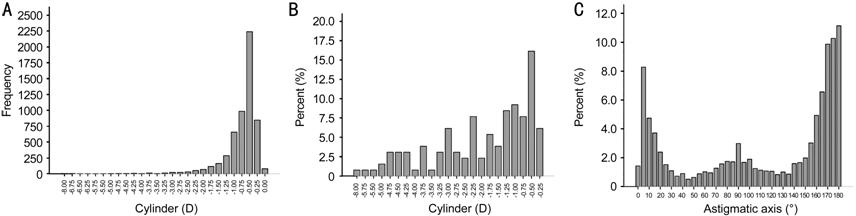
Figure 2 Astigmatic parameters distribution of the
participants in the Shanghai Pudong Eye Study A: Distribution of astigmatism in 5661
measured eyes. Astigmatism was characterized by skewed distribution. B:
Percentage of astigmatism in children (395 eyes) with VA exceed logMAR 0.3; C:
Distribution of astigmatic axis in 5656 measured eyes, mainly astigmatism with
the rule (71%).
DISCUSSION
The specific aims of this study were to measure and
analysis a number of refractive parameters, mainly AL/CRC, to investigate
refractive development characteristics of children in 3 to 4 years age group
based on a large-scale survey, and to provide meaningful data for earlier
diagnosis of vision disorders. According to previous research findings, the
increasingly prevalence and more severe degree of visual disorders in children,
mainly correctable, such as myopia, hyperopia, astigmatism, amblyopia and
strabismus, has become a crucial public health issue worldwide during the past
two decades[2,17-18].
Considering the current status and development of vision disorder of Chinese
children, it is predicable that visual impairment caused by refractive error
and amblyopia in China might be a heavier load, not only for family but also
for society, in the coming future. Effective strategies are needed to eliminate
this situation. The USPSTF recommends at least one vision screening in all 3 to
5y group children to detect amblyopia or its risk factors[19].
This study suggested that the mean AL was 22.10±
The 95%CI of AL/CRC was 2.57 to
The most common refractive error finding in this
study was astigmatism, mainly lower diopter and astigmatism with the rule. The
median of astigmatism was -0.5 D. The most common distribution of astigmatism
in 3 to 4y children was below -0.50 D, accounting for 56.3%, and 85.3% below
-1.00 D. A total of 6.7% for children with astigmatism exceed -1.50 D. However,
only 22.4% under -0.50 D in 395 astigmatic eyes with VA exceed logMAR 0.3, the
majority were over -1.50 D, accounting for 52.3%. Previous studies have shown
that the correlation between AL/CRC and SE is much stronger than that between
cylinder[20]. R2 coefficients
for AL/CRC and SE, cylinder were 0.560 and 0.071, respectively. Meanwhile, most
astigmatism in children has lower diopter. Both of them indicate that astigmatism
has little effect on AL/CRC reference for visual impairment evaluation.
However, this study also found that either degree or proportion of astigmatism
was increased in visual impaired children. Whether or how much impact it would
have to assess visual impairment with AL/CRC reference will be further
researched in subsequent studies. Therefore, using AL/CRC to evaluate
refractive error and VA in children, especially uncooperative children,
astigmatism screening by autorefraction are needed.
There are limitations to our study. First, this study
is a large-scale epidemiological survey with numerous participants therefore
cycloplegic refraction was not carried out. As a result, the correlation
between AL/CRC and diopter cannot be analyzed in this study. However, the main
purpose is to understanding the AL, CRC, AL/CRC, and other refractive
parameters of 3 to 4y kindergarten students, then provide a medical reference
range for refractive development evaluation and earlier visual impairment
screening. Cycloplegic refraction in the hospital is required to confirm the
diagnosis of refractive errors. Second, this study is a school-based study and
restricted to urban areas, nonparticipant might have led to bias.
In conclusion, using AL/CRC reference to assess
refractive development in children and screening uncorrected refractive errors
is practicable and effective. Astigmatism need to be considered in the
diagnosis.
ACKNOWLEDGEMENTS
Foundations:
Supported by
the National Natural Science Foundation of China (No.81371040); Shanghai Smart
Medical Special Research Project (No.2018ZHYL0221); Shanghai Municipal
Education Commission- Gaofeng Clinical Medicine Grant Support (No.20181810);
the Science and Technology Commission of Shanghai (No.17DZ2260100).
Conflicts of Interest: Zhao KK, None; Yang Y,
None; Wang H, None; Li L, None; Wang ZY, None; Jiang F,
None; Qu JF, None.
REFERENCES