IF in JCR CiteScore
Rank About IJO Current
Issue Featured Articles Articles In Press Recent Accepted
 International Journal
of Ophthalmology
International Journal
of Ophthalmology
2017; 10(9):1407-1411
・Clinical Research・
Effects of higher-order aberrations on contrast sensitivity in normal eyes of a
large myopic population
Peng-Fei Zhao1, Shi-Ming Li1,
Jing Lu2, Hong-Min Song3, Jing Zhang1, Yue-Hua
Zhou1, Ning-Li Wang1
1Ophthalmic
Center, Beijing Tongren Hospital, Capital Medical University, Beijing
Ophthalmology and Visual Sciences Key Lab, Beijing 100730, China
2Department
of Ophthalmology, Affiliated Hospital of Hebei Medical University, Baoding
100730, Hebei Province, China
3College of
Applied Arts and Science, Beijing Union University, Beijing 100191, China
Correspondence to: Yue-Hua
Zhou. Ophthalmic Center, Beijing Tongren Hospital, Capital Medical University,
Beijing Ophthalmology and Visual Sciences Key Lab, Beijing 100730, China.
yh0220@ yahoo.com
Received: 2016-01-03
Accepted: 2017-04-17
Abstract
AIM: To
study the relation between higher-order aberrations (HOAs) and contrast
sensitivity (CS) in normal eyes among a population of laser in situ
keratomileusis (LASIK) candidates.
METHODS: In
6629 eyes of 3315 LASIK candidates, CS were measured under dark environment at
the spatial frequencies of 1.5, 3, 6, 12 and 18 cycles per degree (c/d),
respectively, using an Optec 6500 visual function tester. Meanwhile, ocular
HOAs were measured for a 6.0 mm pupil with a Hartmann-Shack wavefront
analyzer.
RESULTS: In
the study, the subjects with an average spherical
equivalent of -4.86±2.07 D were included. HOAs decreased from the third
to the sixth order aberrations with predominant aberrations of third-order
coma, trefoil and fourth-order spherical aberration. At low and moderate
spatial frequencies, CS was negatively correlated with the third-order coma and
trefoil aberrations, and decreased with increasing Z31,
but increased with increasing Z3-3 and Z5-1.
At high spatial frequencies, CS decreased with increasing Z3-3
and increased with increasing Z5-1.
CONCLUSION: At
a large pupil size of 6.0 mm, the third-order aberrations, but not the total
aberrations, are the main factors affecting CS. Vertical coma is negatively
correlated with CS.
KEYWORDS: myopia; contrast sensitivity; higher-order aberrations; coma;
spherical aberration
Citation: Zhao PF, Li SM, Lu J, Song HM, Zhang J, Zhou YH,
Wang NL. Effects of higher-order aberrations on contrast sensitivity in
normal eyes of a large myopic population. Int J Ophthalmol 2017;
10(9):1407-1411
INTRODUCTION
In the past few years, some of the patients had vision degradation with vision blur, glare and halo after laser in situ keratomileusis (LASIK) surgery, and these were considered related to the decrease of contrast sensitivity (CS) after surgery[1-4]. It has been proved that wavefront aberration-guided LASIK can improve CS after surgery[5-8]. Some researchers have studied the relationship between wavefront aberration and CS in small population (the largest sample contains 196 eyes from 112 patients) and they found negative correlation between high-order aberration (HOA) and CS[9-13]. In this study, we studied the relationship between wavefront aberration and CS in a large myopic population (6629 eyes from 3315 patients), our results will provide further evidence to improve wavefront aberration-guide LASIK.
SUBJECTS AND
METHODS
The study
was approved by the Ethics Committee of Beijing Tongren Hospital. Informed
consent was obtained from all individual participants in oral forms and they
did not receive pay in this study.
Subjects The subjects who
visited the Myopia Correction Center of Beijing Tongren Hospital between
January 2006 and May 2011 and planned to receive LASIK were screened. All
subjects should have best corrected visual acuity of 20/20 or better and no
history of eye diseases, trauma or surgery. The difference between manifest
refraction and cycloplegic refraction spherical equivalent was less than 0.50
D. The subjects either had no history of contact lens wearing or stopped
wearing soft contact lenses more than 2wk prior to the ocular examination (or
>8wk if rigid gas permeable contact lens were worn).
Ophthalmic
Examinations Both CS and HOAs were measured in one
dark room by the same technician. CS was examined using an Optec 6500 visual
function tester (Beijing Pratt Medical Instrument Co., Ltd.) with full
correction of refractive errors. A night mode with an illumination level of 3
cd/m2 was used. After closing their eyes and resting for 10min, the
subjects underwent CS examination at 5 spatial frequencies (1.5, 3, 6,
12 and 18 c/d, respectively) with the best corrected
visual acuity. HOAs were measured using a Hartmann-Shack wavefront analyzer (AMO&VISX, USA). After requiring the subjects to blink
their eyes, the image acquisition was finished
within 3s and was repeated for 3 times. The test results
with the best focus on the original picture, the least center deviation, the
smallest lower-order aberration, and the best repeatability of HOA images and root mean square (RMS) values at 6.0 mm pupil
size were included for analysis.
Statistical Analysis SPSS 11.5 software was used for data analysis. Multiple regression analysis and independent samples t-test were used to analyze the data. A P value less than 0.05 indicates a statistically significant difference.
RESULTS
Total 3315
young subjects were included in this study. These LASIK candidates consisted of
611 males (1222 eyes) and 2704 females (5407 eyes) aging from 18 to 40y
(25.95±5.35y). The spherical equivalent ranged from -1.02 D to -10.37 D
(-4.86±2.07 D), and the cylinder from -0.05 to -1.96 D (-0.66±0.47 D).
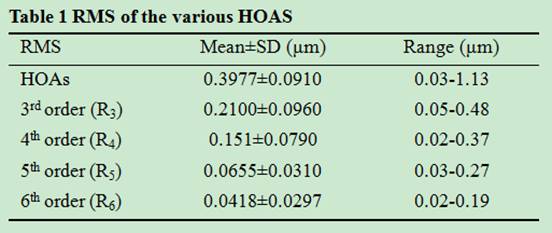
Higher-order
Aberrations At 6.0 mm pupil size, the RMS of the
total HOAs ranged from 0.03 to 1.13 μm, with an average of 0.3977±0.0910 μm.
Among the HOAs, the third- to sixth-order aberrations decreased with increasing
orders. The predominant HOAs were coma (Z3-1-Z31), trefoil (Z3-3-Z33) and fourth-order spherical aberrations (Z40)
(Table 1).
Contrast Sensitivity At the night mode, CS had the maximum of
1.9362±0.1397 at the low spatial frequency of 3 c/d, followed by the medium spatial frequencies of 1.5 c/d
(1.8108±0.1130) and 6 c/d (1.8100±0.1789), and then the high spatial frequencies of 12
c/d (1.1922±0.3000) and 18 c/d (0.5859±0.3300), respectively
(Figure 1).
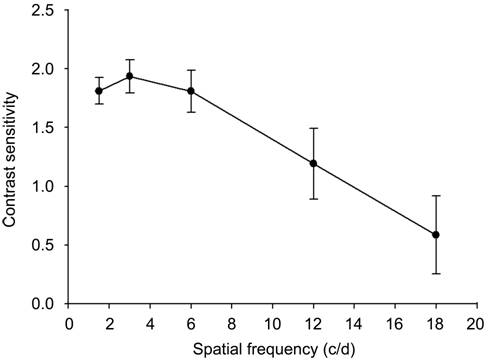
Figure 1 Contrast
sensitivity (mean±SD) of the myopes at different spatial frequencies.
Relation
Between Contrast Sensitivity and Various Orders of Higher-order
Aberrations In these five spatial frequencies (Table
2), we did multiple regression analysis between CS and HOAs. When the spatial
frequency was 1.5 c/d, the regression is
CS=1.7259-0.377R3 (P<0.05). When the spatial was 3 c/d, CS=1.7971-0.7238R3 (P<0.05). When spatial
frequency is 6 c/d, CS=2.0638-0.2215R3 (P<0.05).
These results showed CS decreases when third order aberration increased when
the spatial frequencies were 1.5 c/d, 3 c/d
and 6 c/d respectively.
At high spatial frequencies (12 c/d and 18
c/d), CS was not associated with the 3rd to 6th
order aberrations.

Relation Between Contrast Sensitivity and Various Modes of High-order
aberrations Further multiple regression analysis between CS and various modes of
HOAs showed that CS decreased with the increase of Z31
and increased with the increase of Z3-3 and Z5-1
at the medium (1.5 c/d and 3 c/d) and low (6 c/d) spatial
frequencies. At the high (12 c/d and 18 c/d) spatial frequencies, CS decreased with the increase of Z3-3
and increased with the increase of Z5-1. The regression
equations were examined by F-test and all the P values were less
than 0.05 (Table 2).
Comparisons
of Aberrations Between the High and Low Contrast Sensitivity Group The subjects
were divided into two groups according to the mean CS at each spatial
frequency. Group 1 included subjects whose CS was lower than the mean value,
and Group 2 with CS higher than the mean value. The total aberration, total
HOAs, and third-order to sixth-order aberrations were compared between the two
groups. The results showed that, when the spatial frequency was 1.5 c/d and 3
c/d, the total aberration (R), R3, Z3-3, Z31
and Z5-1 were significantly different between the high
and low CS groups (P<0.05). R was lower in Group 1 than in Group 2. R3 and
Z31 were higher in Group 1 than that
in Group 2, while Z3-3 and Z5-1 were lower in Group 1 than that in Group 2 (Figure 2). When the
spatial frequency was 6 c/d, Z31, Z3-3,
Z5-1, and Z6-2 were significantly different
between the two groups (P<0.05). Z31
was higher in Group 1 than that in Group 2, while Z3-3,
Z5-1 and Z6-2 were lower (Figure
3). When the spatial frequency was 12 c/d and 18 c/d, Z3-3
and Z5-1 were significantly
different between the two groups (P<0.05). Z3-3
was higher in Group 1 than that in Group 2 while Z5-1
was lower (Figure 4).
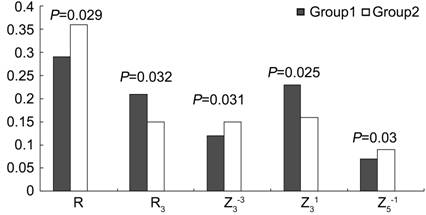
Figure 2
Comparison of CS (1.5 c/d and 3 c/d) between Group 1 and Group 2.
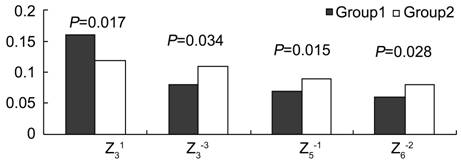
Figure 3
Comparison of CS (6 c/d) between Group 1 and Group 2.
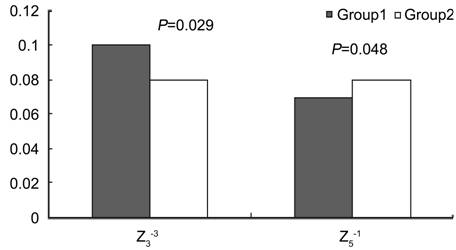
Figure 4
Comparison of CS (12 c/d and 18 c/d) between Group 1 and Group 2.
DISCUSSION
With the
development of refractive surgery, people focused more and more on the visual
quality rather than the naked eye vision only, CS is an important criterion for
measuring visual quality. Human eye is a complicate optical system with
different aberrations and these aberrations are some of the limiting factors of
visual quality[14-17]. Traditional
LASIK surgery can improve naked eye vision but there are some problems after
surgery, including decrease of CS, night glare and decrease of low contrast
vision. Recent studies[1,18-20] have proved these problems are related to HOAs after surgery.
Therefore, wavefront aberration-guided customized ablation is becoming the hot
topic of the corneal refractive surgery[5,21-22]. Researchers have tried to minimize HOA, improve
visual quality and CS by using customized surgery. However the results show
very limited visual quality improvement[23-25]. To solve this problem, we need
to understand the relationship between CS and HOA.
In the
present study, we chose CS as an indicator of visual quality. The subjects were
examined with the best corrected visual acuity then HOAs are relatively
dominant. Multiple regression analysis between CS at five spatial frequencies
and various order aberrations showed that CS at low and medium frequencies
decreased with increasing 3rd order aberrations, but not the total
HOAs. It meant that 3rd order aberrations are the main factor
affecting CS at low and medium frequencies. Multiple regression analysis
between CS at five spatial frequencies and various modes HOAs showed that Z31,
Z3-3, and Z5-1
were the main components of HOAs affecting CS. At low to medium frequencies, CS
decreased with the increase in Z31 and increased with the increases in Z3-3
and Z5-1. At high frequencies,
Z3-3 and Z5-1
also affected CS but with a reversal negative effects
of Z3-3. The other component Z5-1 had consistent positive effects on CS at high frequencies,
similar to its effects on CS at low frequencies. It seems that different
components of 3rd order aberrations played different roles in
affecting CS at different spatial frequencies and their combined effects
deteriorate CS.
It is interesting that not all HOAs reduced CS on human eye. Some components of HOAs, such as Z3-3 and Z5-1, may improve CS at least at low to medium spatial frequencies. It indicates that the effects of individual aberrations might be different from the combined effects of individual aberrations. Various components of HOAs interact with one another[26]. Overall, Z31 and Z3-3 play a major role in affecting CS. That result is consistent with Feizi and Karimian[9] report that when the dark-adapted pupil was large, the third-order coma aberration was the main factor affecting CS.
Comparative
analysis of the aberrations in the high and low CS groups showed that the total
aberration of the two groups was significantly different at low spatial
frequencies, and that the total aberration in the low CS group was lower than
that in the high CS group. Our results were consistent with Lu et al’s[13] study results, but differed from some other reports
in the literature[27-29]
showing that the greater the aberrations, the lower the CS. The third-order
aberrations Z3-3, Z31 and Z5-1 were significantly different between the two groups when the
specific components of aberrations were compared. The aberration component Z31 that can decrease CS was significantly higher in the low CS
group than in the high CS group, leaving the aberration components Z3-3
and Z5-1 that can increase CS
significantly lower than those in the high CS group. The total third-order
aberrations that mainly affect CS at low frequencies were also higher than in
the high CS group. Therefore, although the total aberration in the low CS group
was small, aberrations contained relatively higher numbers of components that
can decrease CS; thus, CS was low.
At medium
and high spatial frequencies, although there was no significant difference
between the two groups in the total aberration, the total aberration in the low
CS group tended to be higher than that in the high CS group. At medium spatial
frequencies, Z31, Z3-3, Z5-1
and Z6-2 were significantly
different between the two groups, and in the low CS group the aberration component
Z31 that can decrease CS was
nonetheless significantly higher than in the high CS group, leaving the
aberration components Z3-3, Z5-1 and Z6-2 that
can increase CS significantly lower. At high spatial frequencies, Z3-3
and Z5-1were significantly different
between the two groups. Z3-3
can reduce CS, and therefore Z3-3 was significantly higher in the low CS group than in the high
CS group, leaving the aberration component Z5-1 that can increase CS lower in the low CS group than in the high
CS group.
Thus, the
total aberration is not a main factor determining the level of CS. Significant
total aberration does not necessarily mean CS will be low; and the composition
of aberration plays a key role. This also suggests that we should not blindly
pursue reduction of the total aberration during wavefront aberration-guided
individualized ablation. Instead, we should choose to reduce the aberration
components that can decrease CS, such as third-order coma and fifth-order
higher-order coma.
In summary,
the relationship between HOAs and CS is complex. Third-order aberrations are
the main factors affecting CS, and the third-order coma can reduce both CS and
visual quality. We cannot simply assume that all aberrations will lower CS and
that elimination of aberrations will improve visual quality. The total
aberration is not the main factor determining the level of CS. The various
components of HOAs may have individual effects different from their combined
effects. Some aberrations may counteract one another. Simple reduction of some
aberrations may break this “balance” among them, reducing visual quality
instead.
ACKNOWLEDGEMENTS
Conflict of
Interest: Zhao PF,
None; Li SM, None; Lu J, None; Song HM, None; Zhang J,
None; Zhou YH, None; Wang NL, None.
REFERENCES
1
Yamane N, Miyata K, Samejima T, Hiraka T, Kiuchi T, Okamoto F, Hirohara Y,
Mihashi T, Oshika T. Ocular higher-order aberrations and contrast sensitivity
after conventional laser in situ keratomileusis. <ii>Invest Ophthalmol
Vis Sci</ii> 2004;45(11):3986-3990. [CrossRef]
[PubMed]
2
Zhang J, Zhou YH, Li R, Tian L. Visual performance after conventional LASIK and
wavefront-guided LASIK with iris-registration: results at 1 year. <ii>Int
J Ophthalmol </ii> 2013;6(4):498-504. [PMC free article] [PubMed]
3
Loukotova V, Vlkova E, Horackova M, Tokosova E, Pirnerova L, Hlinomazova Z,
Dvorakova D, Nemec J. Changes of higher order aberrations and contrast
sensitivity after standard photorefractive keratectomy. <ii>Cesk Slov
Oftalmol</ii> 2009;65(5):176-181. [PubMed]
4
Oshika T, Tokunaga T, Samejima T, Miyata K, Kawana K, Kaji Y. Influence of
pupil diameter on the relation between ocular higher-order aberration and
contrast sensitivity after laser in situ keratomileusis. <ii>Invest
Ophthalmol Vis Sci</ii> 2006;47(4):1334-1338. [CrossRef]
[PubMed]
5
Jahadi Hosseini SH, Abtahi SM, Khalili MR. Comparison of higher order
aberrations after wavefront-guided LASIK and PRK: one year follow-up
results<ii>. J Ophthalmic Vis Res</ii> 2016;11(4):350-357. [CrossRef]
[PMC free article] [PubMed]
6
Marcos S. Aberrations and visual performance following standard laser vision
correction. <ii>J Refract Surg</ii> 2001;17(5):S596-601. [PubMed]
7
Ang RE, Reyes KB, Hernandez JA, Tchah H. Wavefront-guided epithelial laser in
situ keratomileusis with mitomycin-C for myopia and myopic astigmatism: flap-on
versus flap-off technique. <ii>J Cataract Refract Surg</ii>
2011;37(6):1133-1139. [CrossRef]
[PubMed]
8
Hatch BB, Moshirfar M, Ollerton AJ, Sikder S, Mifflin MD. A prospective,
contralateral comparison of photorefractive keratectomy (PRK) versus thin-flap
LASIK: assessment of visual function. <ii>Clin Ophthalmol</ii>
2011;5:451-457. [PMC free article] [PubMed]
9
Feizi S, Karimian F. Effect of higher order aberrations on contrast sensitivity
function in myopic eyes. <ii>Jpn J Ophthalmol</ii>
2009;53(4):414-419. [CrossRef]
[PubMed]
10
Oshika T, Okamoto C, Samejima T, Samejima T, Tokunaga T, Miyata K. Contrast
sensitivity function and ocular higher-order wavefront aberrations in normal
human eyes. <ii>Ophthalmology </ii>2006;113(10):1807-1812. [CrossRef]
[PubMed]
11
Tanabe T, Miyata K, Samejima T, Hirohara Y, Mihashi T, Oshika T. Influence of
wavefront aberration and corneal subepithelial haze on low-contrast visual
acuity after photorefractive keratectomy. <ii>Am J Ophthalmol</ii>
2004;138(4):620-624. [CrossRef]
[PubMed]
12
Seiler T, Kaemmerer M, Mierdel P, Krinke HE. Ocular optical aberrations after
photorefractive keratectomy for myopia and myopic astigmatism. <ii>Arch
Ophthalmol</ii> 2000;118(1):17-21. [CrossRef]
14
Schwiegerling J. Scaling pseudo-Zernike expansion coefficients to different
pupil sizes. <ii>Opt Lett </ii>2011;36(16):3076-3078. [CrossRef]
[PubMed]
16
Serrao S, Lombardo G, Ducoli P, Lombardo M. Long-term corneal wavefront aberration
variations after photorefractive keratectomy for myopia and myopic astigmatism.
<ii>J Cataract Refract Surg</ii> 2011;37(9):1655-1666. [CrossRef]
[PubMed]
17
Jungnickel H, Babovsky H, Kiessling A, Gebhardt M, Grein HJ, Kowarschik R.
Effects on vision with glare after correction of monochromatic wavefront
aberrations. <ii>J Refract Surg </ii>2011;27(8):602-612. [CrossRef]
18
Liu TX, Chen YT, Dan TT, Shi R, Linghu SR, Li HX. Four-year follow-up of
corneal aberrations and visual functions of myopic patients after laser in situ
keratomileusis. <ii>Pak J Med Sci </ii>2015;31(6):1453-1456. [CrossRef]
[PMC free article] [PubMed]
19
Khan MS, Humayun S, Fawad A, Ishaq M, Arzoo S, Mashhadi F. Effect of wavefront
optimized LASIK on higher order aberrations in myopic patients. <ii>Pak J
Med Sci</ii> 2015;31(5):1223-1226. [CrossRef]
[PMC free article] [PubMed]
20
Chan JW, Edwards MH, Woo GC, Woo VC. Contrast sensitivity after laser in situ
keratomileusis. one-year follow-up. <ii>J Cataract Refract
Surg</ii> 2002;28(10):1774-1779. [CrossRef]
21
Moussa S, Dexl AK, Krall EM, Arlt EM, Grabner G, Ruckhofer J. Visual,
aberrometric, photic phenomena, and patient satisfaction after myopic
wavefront-guided LASIK using a high-resolution aberrometer. <ii>Clin
Ophthalmol</ii> 2016;10:2489-2496. [CrossRef]
[PMC free article] [PubMed]
22
Ye MJ, Liu CY, Gu ZY, Zhao BY, Liao Y. SMILE and wavefront-guided LASIK
out-compete other refractive surgeries in ameliorating the induction of high-order
aberrations in anterior corneal surface. <ii>J Ophthalmol
</ii>2016;10:870-876. [CrossRef]
24
Mrochen M, Kaemmerer M, Seiler T. Wavefront guided laser in situ
keratomileusis: early results in three eyes<ii>. J Refract Surg
</ii>2000;16(2): 116-121. [PubMed]
27
Sakata N, Tokunaga T, Miyata K, Oshika T. Changes in contrast sensitivity
function and ocular higher order aberration by conventional myopic
photorefractive keratectomy. <ii>Jpn J Ophthalmol</ii>
2007;51(5):347-352. [CrossRef]
[PubMed]
28
Hiraoka T, Okamoto C, Ishii Y, Kakita T, Oshika T. Contrast sensitivity
function and ocular higher-order aberrations following overnight
orthokeratology<ii>. Invest Ophthalmol Vis Sci</ii>
2007;48(2):550-556. [CrossRef] [PubMed]
29
Stoimenova BD. The effect of myopia on contrast thresholds. <ii>Invest
Ophthalmol Vis Sci</ii> 2007;48(5):2371-2374. [CrossRef]
[PubMed]